Comfort Etim from Refugee Women Connect speaks to the Demonstration from atop the FBU appliance at the start of the demonstration, about the importance of Saving Liverpool Women’s Hospital .
Comfort Etim on the left of the picture with Aliya, Nakki and Nina
Reasons to Save Liverpool Women’s Hospital
“When asked to speak today, I ask myself why and what change do I want to see. The answer is change the narrative and join in solidarity to Save the Women’s Hospital where I have been privileged to have two of my children and I don’t think merging it is the right thing to do.
Speaking to over 20 women about why the women’s hospitals is important to them they all echoed the same thing as it is a safe space for women and should remain open where it is.
As mentioned, I work for Refugee Women Connect which is a charity organization that provides support for women seeking asylum, refugees, and survivors of trafficking across Merseyside.
We have continued to work we the women’s hospital in improving information around asylum and how best staff can continue to understand how to care for women having babies in the asylum system and be more welcoming and we believe the space has been created there is the capacity for it here at the women’s hospitals and fear it will be completely lost if we move the women’s hospitals to the Royal.
We love all the staff here at the women’s hospitals as they have welcomed us, listened to us, and continued to work with us. Our women feel very comfortable coming to the Women’s to have their babies just like I felt coming here to have my babies and we don’t want that to change.
The Migrant Surcharge
Next year the NHS Surcharge goes up and this will impact a lot of women. Migrant have been paying a lot of money to assess care in the UK and so when the government say things like we will increase visa and NHS charge it sounds as though it is a new thing but it is not.
The gaps in the NHS can be changed to an extent if the government could allow asylum seekers to work (Joining the campaign Lift the Ban) there are doctors, nurses, midwives, teachers, and many skilled workers amongst them.
If given the right to work they too can contribute to the society and thrive in a place they now call home.
The purpose of establishing women’s hospitals in the UK is to provide specialized healthcare services tailored to the unique needs of women. By having separating the women’s hospitals, healthcare providers can offer comprehensive care, conduct research, and promote education and awareness about women’s health in a safe place.
In summary, we stand in solidarity with the NHS staff for good pay and an improved support system for them to continue the amazing work they are doing already.
They need more staff to join the work, give asylum seekers the right to work so that they can reduce the workload, and contribute to our economy. Take away two and half years visas so that young children and adults wanting to further their education in healthcare can gain admission into universities.
Say loud say it clear refugees are welcome here. Refugee Women Connect believes Solidarity knows no border.”
Additional Note from Save Liverpool Women’s Hospital Campaign.
The Migrant charge for NHS services is an annual charge imposed on migrants. Migrants paying this charge can then use the NHS services as others do but not every migrant can use this system and face very harsh charging
Every pregnant woman should have maternity care free of charge. We have campaigned against the different kinds of migrant charges for the NHS. It is a bad system for pregnant women and has cost lives of mothers and babies
“Until the increased rates take effect in 2025, the UK Immigration Health Surcharge currently costs £624 per applicant per year of leave granted, or a £470 per year discounted rate applies for student visa holders, those on the Youth Mobility Scheme and children under the age of 18.” So more than £2,000 for a family of 4.
The government cannot play ignorance. Their Chancellor Jeremy Hunt has been deep in the reorganisation of the NHS on US lines for years.
The government is provoking a huge crisis as we head into a winter of avoidable deaths and harm. It will make a pretty penny for the big corporations though.
This is widely expected to be followed by a merger pulling women’s health, genetics, fertility, and maternity into a huge conglomerate.
Chief Executive of the Liverpool Women’s Hospital is the top Maternity job in the country. Maternity is in a national crisis of staffing and safety. Why won’t Mr Sumner tell us what he knows about Maternity?
Repeatedly, we see reports of inadequate care in maternity across the country. Most recently
“Maternity services at Royal Derby Hospital and Queens Hospital, part of University Hospitals of Derby and Burton, were inspected by the CQC in August as part of the regulator’s national maternity services inspection programme, which has seen an increasing number of maternity services across the English NHS rated “inadequate.”
Liverpool Women’s Hospital claims to be the only fully staffed maternity provider in the country, though many of the midwives are newly qualified. We do hope those midwives stay!
It seems that the axe will not fall on maternity as hard as it will on other services.
Dr Suzanne Tyler, Executive Director of Trade Union at the RCM, said:
“While we acknowledge that this will be an incredibly difficult time for our colleagues elsewhere in the NHS, we are grateful that NHS England has listened to our plea to maintain the level of funding and investment in maternity services to protect safety. To have done otherwise would have been incredibly damaging to the ability of midwives, maternity support workers and other maternity staff to deliver safe care to women and families. We already know the impact that can have, and we are pleased to be working with Trusts and others to bring about positive change. This commitment to the continuation of funding should not be underestimated and we strongly urge Trusts to honour this commitment.
“Recent reviews by Dr Bill Kirkup and Donna Ockenden have called on the Government and on NHS bodies to address the chronic maternity workforce shortage and to invest in the safety of services. We hope that today’s announcement will go some way to make those recommendations a reality.”
Our campaign says “maintaining” current levels is not good enough and damaging the rest of the NHS is simply wrong Women need heart care, diabetes care, mental health care as well as maternity care and they all intertwine. Stop this government’s health policies in their entirety.
Women are being damaged.
Women, and especially mothers, are being damaged by poverty, the housing crisis cold homes and poor pay. Becoming a mother is very tough for many. A recent report shows young mothers are especially vulnerable.
Join your voices for our health care. Demand it back.
Restore and Repair the NHS. Stop the rot now!
Profit-centred policies are reshaping and downscaling our health services. These policies are destroying our services. providing fewer services, fewer beds and massive staff shortages. But it provides more profit for health corporations like Optum and management consultants like Carnall Farrar
Privatisation policies are hidden behind sweet words. The privatisation lobby is also infecting Labour, so the fightback is down to us all. The NHS was not a gift from the great and the good but something fought for for years by working class women and by the Trade Nnions. We got the NHS that way and we can get it back the same way
Government policy costs lives., especially the lives of working-class people.
The US system has more preventable deaths than any other advanced country.
What has happened to dentistry and mental health services can happen to every service.
Wages and conditions in the NHS have fallen in real terms. Staff are working way beyond their duties just to keep the service afloat.
We will never get our services back unless we all spread the word.
Don’t be the person who has today to your grandchildren as they struggle to pay for poor health care
“Well we did have a health service for everyone but they privatised it”
One to one conversations build our campaign
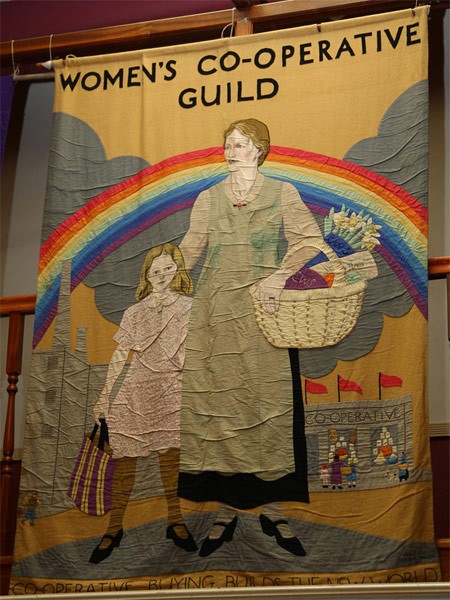
The Women’s Cooperative Guild organised a mass campaign for maternity care for all women
Key facts
•In the US health insurance costs about as much as the family mortgage and does not cover everything. Many go without.
• Private healthcare cannot be as good as a national comprehensive service.
• We pay through our taxes. Government money invested in healthcare pays back into the economy.
Demand a return to the original NHS, once the best in the world. It was Government funded, providing timely healthcare for all, including all the services, publicly delivered by qualified staff with decent pay and conditions. This is how the NHS was designed by Aneurin Bevan, seventy five years ago.
It is the cheapest, most cost-efficient and humane way to provide health care. If YOU spread the word, we stand a chance of getting our services back .
We know we have the support of the people of Cheshire and Merseyside. We work with health campaign groups and trade unions across Cheshire and Merseyside and beyond. We have more than 70,000 signatures on our petition, combining the paper signatures and the online petition. We have distributed tens of thousands of leaflets; three big demonstrations all show this support.
We have a feral government intent on transforming the NHS into a cash cow for big corporations.
We are calling for a winter of protest and campaigns to inform the public. Help us if you can!
At our campaign meeting on November 6th, 2023 we discussed the CQC report on the Liverpool Women’s Hospital, the CQC report on all the maternity providers nationally, infant mortality at the Liverpool Women’s Hospital as reported in the MBRAACE report, the appointment of a joint chair of the board with Liverpool University Hospitals Trust, the cuts imposed by the ICB, the shortages of midwives, obstetricians, and concerns about women’s experience of giving birth. We also discussed our wonderful demonstration on the 7th of October 2023.
Although we discussed all these issues, our conversation kept coming back to the babies and children in Gaza and the hospitals there under the horrific bombing by Israeli forces. We could not ignore the killing of babies and children in Gaza the problems of women giving birth under a rain of bombs, and the terrible state of the health service in Gaza.
Our hearts go out to those who died, all who are injured or bereaved, and to the families of all the children killed injured, or kidnapped, definitely including those killed in Israel by Hamas.
As of 3 November, according to Ministry of Health data, 2326 women and 3760 children have been killed in the Gaza strip, representing 67% of all casualties, while thousands more have been injured. This means that 420 children are killed or injured every day, some of them only a few months old.”
Save Liverpool Women’s Hospital Campaign focuses on the issues around women’s health, maternity, infant mortality, the NHS and NHS staff, restructuring legally and organisationally for privatization, and the diversion of funds to private profit. We focus also on staffing and working conditions, but the situation in Gaza cannot be ignored. Too many women and babies, doctors, and nurses have died.
Liverpool Women’s Hospital itself was attacked by a lone bomber so we know the experience of terror attacks. Mill Road Hospital, one of our predecessors, was bombed during the Blitz and the stories of that incident live on amongst us.
St Luke’s Church, just over a mile from Liverpool Women’s Hospital, stands at the top of Bold Street in memorial to that Blitz and to the demand that such attacks on civilians never happen again, but bombs are raining down on the people of Gaza as they did on Liverpool more than eighty years ago. Around four thousand people in Liverpool died during the blitz according to official figures, but it may have been more. In Gaza, it is ten thousand dead and the bombs are still falling. The United Nations has called it a children’s graveyard.
Just as the stories of the bombing of Mill Road Hospital are still retold today, in eighty years so will the tales of bombing Gaza. For the sake of the survivors in Gaza and Israel, the children must grow up in peace.
For now, the demand must be for a ceasefire.
Our hearts ache for the women giving birth under bombing, lacking proper medical care, and anesthetics. Our admiration goes out to the hospital staff who stay and care for their patients. One report says “Some women experience postpartum bleeding and we can’t manage it… we’ve performed hysterectomies on women who could have been saved. But to save blood, we’ve made the decision to remove the uterus to increase the chances of not losing the patient.” #Gaza.
There was a truce during Christmas in World War 1 commemorated in a statue at St Lukes. A ceasefire is not impossible. It’s a choice to be made by people who were born of women. We join the call for a ceasefire now.
Added on Saturday 11th November morning.We hear that a hospital is now also under full scale land attack and that the power for the incubators has failed.
A message from Sharon Graham General Secretary of Unite the Union
Picture Credit Morning Start Neil Terry
“Friends
What women know from the generations that came before us – from those who stood up and fought for the right to work, good pay and conditions – is that we don’t get what we want just because it is the right thing to do. We have to fight for it.
The Liverpool Women’s Hospital is one of those fights. A jewel in the crown of the NHS that is under attack. A lifeline for women, babies, and families across the North West. It is the sole specialist trust of its kind in the UK, delivering vital care and support.
So of course, I join you in fighting for this institution and rejecting any attempt to dilute or dismantle these services.
And we know that this fight is part of a bigger battle to save our NHS from the forces of capitalism and austerity that have been waged against it for many years.
Never forget – this is a battle we cannot afford to lose.
So be assured – Unite stands with you – everyone here rallying to protect this fantastic institution. Liverpool Women’s Hospital must remain as a beacon for women’s healthcare. We must fight to save it. We must fight to save our NHS. And we must win.
We are not stopping until we win back the full NHS, a health care system that properly values our babies and us as women. For all our mothers, daughters, friends and lovers and for every precious baby.
The latest blow to the future of Liverpool Women’s Hospital is the announcement of a joint chair with the Liverpool University Foundation Hospital trust (this is the merged Royal, Aintree and Broadgreen Hospitals). There was no mention of this at the last Liverpool Women’s Hospital Board meeting held in public, nor at the ICB meeting. Where are these decisions being made?
It is farcical that such an appointment is even considered. Women’s services must be prioritised and maternity must be led by people with deep experience in this matter. It cannot be an afterthought to a huge recently merged hospital system.
What has been and is still happening in maternity nationally can no longer be tolerated. A merger with Liverpool’s big merged hospital will not address these issues. The major reports on these issues are authoritative and powerful. The Government’s tactics are to publish and ignore the reports or issue a series of directives that are not backed by finance or staffing.
Maternity has not been given priority in the big merged hospitals, so favoured by this government. Women’s health has not been given its due importance in these merged hospitals either. We have previously quoted the mantra of the priorities for operating theatre as being Life, Limb, and Testicles.
Following Shrewsbury, the site of the first Ockendon report into unnecessary baby deaths, the NHS hospitals had to be told to have a maternity rep on each board. Maternity must not be a second-class, Cinderella service. Ockendon and other reports have shown how deeply damaged NHS maternity has become in this era of bureaucratic management. The reports describing the problems in these services are detailed, authoritative, and ignored. The Birmingham Hospital regularly hyped as the model by those who wish to merge Liverpool Women’s Hospital with the Royal/LUHFT was recently described as showing misogyny and medical patriarchy
We campaign for the restoration of the whole NHS, to get it back from the big corporations and their advocates who are damaging it. Maternity and women’s health issues need to be embedded into the whole health service, damaged as it is, and given greater, not less priority.
We campaign for Liverpool Women’s Hospital as
a women’s hospital,
a provider of services in the community,
a maternity hospital, and
a maternal medicine center,
an NHS hospital, publicly provided for everyone free at the point of need, linked to the whole national health provision,
and an excellent employer.
We have held three demonstrations, gathered more than 73,000 petition signatures, run stalls, attended meetings, gained the support of Kim Johnson the local MP, and others, had resolutions agreed upon at Liverpool City Council, gained support from local and national trade unions, met with the ICB, attended LWH board meetings for many years, run this blog and social media, attended academic and campaigning conferences, put up banners and posters and worked with many other campaign groups. All this, it seems is not enough to gain consultation.
The background to our struggle is both the damaging political reorganisations in the NHS and the consequential maternity scandals that have rocked this country. The dismantling of the NHS, transforming it into a for-profit system, and hence for the adoption of the American Accountable Care system, known here as the ICB (It is used in the US to administer second-class, state-funded healthcare). The private companies administering this get their huge profit by denying care). In the UK, it means fewer hospital beds, fewer staff, closed and merged hospitals, and money being the driving force in service provision. For more details see an earlier post here.
Despite promises both verbal and written of consultation, there was an announcement this week, without consultation with the public, that the chair of Liverpool Women’s Hospital is to be advertised as a joint position with the chair of Liverpool University Hospitals Trust. It was announced to the staff of LUHF T today and in a letter to some others.
Liverpool Women’s Hospital is the largest maternity Hospital in England. It is a maternal medicine centre and a referral hospital. It is a unique Women’s Hospital providing care for women at a time when women’s health is suffering. It provides care for some of the most vulnerable women and babies.
Like all maternity care, it has been underfunded and reorganized to fit the government’s ideology. Even when it meets the government’s staffing ratios we firmly believe that is insufficient for high-quality care.
Maternity nationally is a service struggling with cuts, poor reorganizations, staff shortages, poor working conditions, poor pay and staff attrition.
Two-thirds of England’s maternity units are dangerously substandard says the Care Quality Commission
CQC says too many mothers and babies receive care that is not good enough, with staff shortages among the reasons.
Almost two-thirds of maternity units provide dangerously substandard care that puts women and babies at risk, the NHS watchdog has said in a damning report.
The Care Quality Commission (CQC) has rated 65% of maternity services in England as either “inadequate” or “requires improvement” for the safety of care – up from 54% last year.
Services are beset by a host of problems, including serious staff shortages and internal tensions, which mean that too many mothers and their babies receive care that is not good enough.
Liverpool Women’s Hospital also had a highly critical CQC report, and this was despite the hard work of its staff. The UK does not match other developed countries in infant mortality or maternal mortality.
The board at Liverpool Women’s Hospital spoke about challenging the CQC report describing all their efforts to keep to regulations. We say in challenge to this that the regulations do not in themselves keep babies or women safe. That requires respect for women and babies, sufficient staff and good working conditions.
The CQC report on Liverpool Women’s said
“Liverpool Women’s NHS Foundation Trust is a specialist trust that specialises in the health of women, babies, and their families. It is one of only two specialist trusts in the UK and the largest women’s hospital in Europe. As a tertiary centre the hospital provides care for a significant proportion of patients with high levels of complexity and clinical risk, as well as serving a local population with significant deprivation. The hospital teams deliver around 8,000 babies and perform some 10,000 gynaecological procedures each year.
The trust is situated in an area where 44% of the population live in the lowest quintile for deprivation in England. 26% of children (0-15 years) live in poverty. The region performs significantly worse for premature cancer, cardiovascular disease (CVD) and respiratory deaths. 46% of women booking with Liverpool Women’s Hospital are from the 1st decile on the deprivation index, compared to a national average of 13%
The CQC report said
Following our inspection, we issued a warning notice requiring the trust to make significant improvements.
The trust must assess and do all that is reasonably practicable to mitigate risks to the health and safety of women, birthing people, and babies. Regulation 12 (1)(2)(a)(b) This includes but is not limited to:
Timely and effective triage of women and birthing people
The trust must ensure they deploy sufficient, suitably qualified midwifery staff across all areas of the service. Regulation 18 (1)
Assessing, documenting, and responding to ongoing risks to the safety of women, birthing people, and babies at allstages of pregnancy in line with national guidance Our findings 5 Liverpool Women’s NHS Foundation Trust Inspection report
The trust must ensure staff are up to date with mandatory training. Regulation 12 (1)(2)(c)
The trust must ensure there are sufficient numbers of suitably qualified, competent medical staff to deliver the service and reduce delays in medical review in maternity triage.. Regulation 18 (1)
The trust must ensure it operates effective systems and processes to assess, monitor and improve the quality ofservices and mitigate the risks to women, birthing people, and babies. Regulation 17 (1)(2)(a)(b) This includes but is not limited to:
The reporting and management of patient safety incidents
Receiving and acting on feedback from women, birthing people, families, and staff
Operating robust governance processes
Taking action to improve perinatal mortality rates
Taking timely and effective action to address risks and improve performance
Operating a robust risk register, with effective mitigation and controls and updated action plans
Collecting reliable data to analyze and improve performance
Operating effective audit processes
The hospital does indeed spend time keeping to regulations, juggling how and where it uses staff.
Birthrate Plus is not enough. It is though,our view that the basic government criteria are inadequate. We need more than that, especially but not exclusively in the areas of high deprivation.
Maternity needs to be able to win back some of the staff who have left, to keep the newly qualified staff, (and LWH do seem to be doing that), to be generously funded, and to be able to provide care at least as well as other advanced countries. Once we were the best health service in the world… We can be that again.
Sharon Graham from Unite the Union said at our demonstration on October 7th,
October 7th demonstration to Save Liverpool Women’s Hospital
“What women know from the generations that came before us – from those who stood up and fought for the right to work, good pay and conditions – is that we don’t get what we want just because it is the right thing to do. We have to fight for it.”
Our campaign will continue. Please join us in fighting for Women’s health, and maternity and for the restoration of the NHS as a publicly owned, publicly delivered, not-for-profit health system.
Thank you – it’s a pleasure to be here today and I would like to thank the organisers for giving me the opportunity to talk about what’s happening to our NHS.
We’re all here because we believe in the NHS as a:
comprehensive
Universal
publicly owned
and publicly delivered service
and because we know we must fight for its future.
We know that the NHS is in crisis – and it’s a crisis of the government’s own making.
Waiting lists for routine treatment recently hit record highs of 7.68 million.
And there are well over 100,000 staffing vacancies across the NHS.
Many nurses, midwives, doctors, ambulance workers and other dedicated NHS staff are over-stretched and facing burnout.
Meanwhile, the government continues to underfund the service and increase opportunities for private health companies to make profits off the back of people’s ill health.
The Tories’ undermining of the NHS is a political choice – and they are being found out.
Earlier this year, the highly respected Professor Sir Michael Marmot said:
“If you had the hypothesis that the government was seeking to destroy the National Health Service…all the data that we’re seeing are consistent with that hypothesis.”
When asked if we are stumbling or sleepwalking towards a privatised health care system, he added that government ministers are “not behaving as if they want to preserve our NHS.”
That is a damning indictment of the Tory government.
We should not be surprised, because, the truth is, the Tories have made no secret of their desire to privatise the NHS over decades.
In 1988, John Redwood and Oliver Letwin wrote a pamphlet which has been seen by many as a blueprint for the privatisation of the NHS.
Fast forward 20 years to 2008 and Jeremy Hunt, now the Chancellor of the Exchequer, co-authored a book which included the line: “Our ambition should be to break down the barriers between private and public provision, in effect denationalising the provision of healthcare in Britain.”
The Tories have two tactics when it comes to destroying our NHS.
One is to legislate to open it up to greater privatisation, and the other is to starve it of funding.
One of the key measures in the 2012 Health and Social Care Act was to allow NHS Foundation Trusts to, in effect, earn 49% of their income from treating private patients.
This is wholly unacceptable.
The 2022 Health and Care Act created 42 statutory Integrated Care Boards and Integrated Care Partnerships.
The latter are able to include representatives of private companies, yet they are tasked with preparing the integrated care strategy for an area.
This integrated care strategy sets out how the assessed needs in relation to an area are to be met by the exercise of functions of the Integrated Care Board, which is the commissioning body.
This is outrageous.
There should be no private interests influencing where public money is spent on health and care.
And there should be no room for conflicts of interest.
ICSs have been designed to be vehicles for cuts.
In May, it was reported that ICSs will have to make average efficiency savings of almost 6% – the equivalent of £6 billion across England – to meet their financial requirements this year.
For Cheshire and Merseyside, the ‘efficiency’ target for this year is 5% – or £57.9 million.
How can the NHS in Cheshire and Merseyside make cuts of £57 million when waiting lists are sky-high and there are insufficient staff?
How can the needs of patients be met?
The simple answer is: they can’t be. And they can’t be because of political choice.
It doesn’t need to be this way.
If the government continues to underfund the NHS, increasing numbers of patients will be left, in pain and anxiety, without treatment.
And some will be so desperate they will pay to go private and pay for services which they are entitled to receive free of charge on the NHS.
So I want to finish with this:
Our NHS is in jeopardy.
The government is starving it of resources – and patients and staff are paying the price.
The next government must prioritise the NHS by giving it the significant increase in funding that it needs, and it must put an end to privatisation.
Without a commitment to the NHS as a well-resourced public service, our NHS will not survive.
So it’s vital we continue our fight to save our National Health Service.
I would like to thank each and every one of you for keeping the faith and keeping up the fight. Together we can – and will – save our NHS.
Mary Whitby – contribution at the SLWH rally at the Old Stone Arch, 7 October 2023
Good afternoon
I wanted to dispel some myths.
Mary describes whats happened to the NHS
The NHS is not overwhelmed because we are all using it too much or because of so-called bed blockers nor because we are an aging population – we didn’t just beam down from Mars overnight!
Nye Bevan said our ill health is not a commodity from which they should profit and yet even our our health records are up for sale.
Its not overwhelmed because we cannot afford to run a first class health service for all nor because of covid, asylum seekers or migrants nor because staff have had enough of a decade of pay cuts and have decided to take industrial action.
Mary Whitby making our case with Sharon Graham General Secretary of Unite the Union
So that’s just some of the myths.
The private sector lobbyists are funding political parties and politicians and so those parties make their policies reflect the demands of those private profiteers. Managers and politicians, including on the left, have been told the restructuring of the NHS was necessary as a response to supposedly changing needs. Labour complain its just a matter of low resources.
These myths serve to drown out the reality that the NHS has been carved up and shrunken to open up the space for the private sector to benefit.
In order to make money out of the NHS, providers take contracts to provide shrunken services at great cost to the public purse, employing fewer, less qualified staff, on lower pay hence why there are 130,000 unfilled vacancies.
When our NHS filled the space and our needs were met, we didn’t need to bother with the private sector, why would we pay again for something when we had the NHS which provided what we needed for free when we needed it?
So the private sector couldn’t get a foothold. They couldn’t compete with district general hospitals and family GPs. Successive governments of all parties have played their part in the break up of the NHS, allowing privateers to be embedded inside the NHS remodelling it
Worst of all we never voted for this
So that visual demonstration – if you shrink the NHS it stands to reason it can’t treat as many people as it did before. So even if we didn’t grow older, didn’t have any more babies then the NHS could not cope. They have closed tens of thousands of beds, closed hospitals and 125 A&Es so it is no wonder there are queueing ambulances, trolleys in corridors, people waiting 24 hours in A&E, virtual wards, people unable to get a GP appointment or a scan or 7.7m people suffering on waiting lists.
This is what we mean when we talk about the denial of care.
It is not the NHS model which can’t cope though, it’s the 42 separate American Integrated Care Systems which have caused this crisis which is set to worsen again this winter.
What does 7.7m people on waiting lists look like? If you add up all the populations of the 14 biggest cities in the country then it still doesn’t add up to 7,700,000 people! (Since writing this speech that figure has increased to 7,800,000 people)
To demonstrate how the NHS has been undermined, I have an assistant to help, he will stand over there away from the electrical equipment because I don’t want to be responsible for blowing up the mics and sending the Fans Supporting Foodbanks gazebo up in flames! – imagine there is a pint of beer in this pint glass.
What happens if you try to pour a pint of beer into a half pint glass?
Yes! It overflows because it’s a physical impossibility to fit the same amount of beer into a glass which is half the size and so it is with what’s left of our health service. There are the same amount of patients but the capacity of the NHS to meet our needs has been drastically reduced.
So all the beer overflowing from the glass represents the 7.7m people on waiting lists, it represents all the public NHS funding which never reaches frontline services or staff pay packets but is siphoned off into private pockets, its the staff leaving the NHS, it is all those people who die unnecessarily every week, it represents all those people forced to get into debt and go private to get the medical care they desperately need.
Health is a multi billion dollar commodity and our ill health will be bought and sold if we don’t fight.
In the 5th richest country in the world, we can afford a high-class NHS. In fact, we can’t afford not to have one unless we want to pay with our lives and the lives of the generations to come after us.
So we want you to join our movement to raise awareness in your friends, family, and workplaces in your union branches and communities, have those conversations, spread the word and encourage everyone to become active. As Nye Bevan said the NHS will last as long as there are people willing to fight for it.
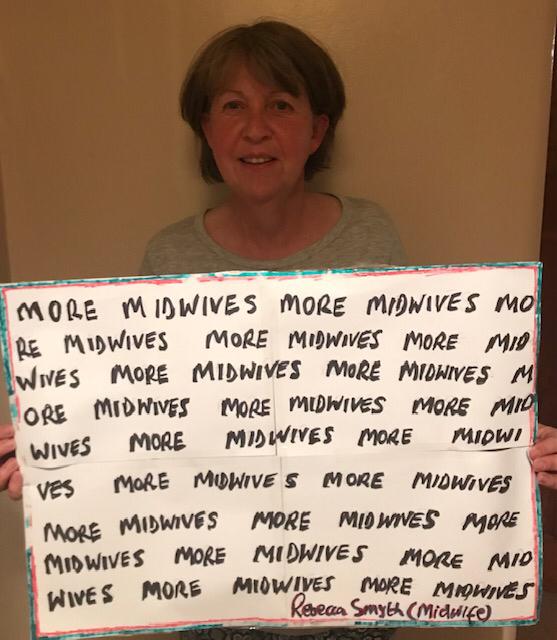
We need more midwives, more midwives and to keep the midwives that we have now.
Rebecca Smyth spoke at the demonstration to Save Liverpool Women’s Hospital on Saturday, October 7th. We had excellent weather and a good turnout. We will be publishing all the speeches.
Hello everyone,
I worked for 35 years as a midwife, and a nurse before that. I’m also an active member of Save the Liverpool Women’s Hospital Campaign group.
I’m wanting to tell you what is happening in midwifery and maternity care. I’ve never known a time when Midwifery is under such threat. Midwifery is a profession almost entirely of women, providing care for women and here we are outside the Liverpool Women’s Hospital and all 3 are at risk; the midwives, the women AND the hospital.
Let me tell you how it is in midwifery now and about the crisis in maternity and why I believe the moving of the hospital will worsen the situation for Midwives and of course the women, babies and families that are cared for.
Now our understanding at the moment is that the hospital will move to the new Royal Hospital site…. Can you imagine that?! And we are campaigning to keep the hospital here.
To understand how catastrophic this is, I want to tell you about the crisis in maternity that we’re experiencing now.
Well in a nutshell there aren’t enough Midwives, the official figures say we are 3,500 short. If you haven’t got enough midwives then the services you provide are not safe.
Without midwives childbirth is at risk,
without midwives families are not safe,
without midwives women don’t get the care they need and deserve.
Because, how can you give safe care when they’re just aren’t enough of you?
And why aren’t there enough midwives?
Well, Midwives are leaving in their droves; and that’s because morale is at rock bottom, midwives are overworked and completely exhausted. They are working in an environment that often isn’t safe. So, many leave… either retiring early (like me), reducing their hours, changing careers completely, or leaving for no job at all.
And the reasons they are giving are insufficient staff numbers, burnout and stress.
Rebecca speaking from the Fire Brigades Union Campaign wagon
They are literally on their knees.
The consequence of this, is that there is not one maternity unit in the country that is adequately staffed. That’s every day, that’s today, that’s now.
Not a day goes by when we do not hear about a maternity unit closing its doors and women being sent to other hospitals. Did you ever imagine the day would come when you would hear that a hospital closed its doors? That is what shops do, that is how businesses are run. Yes, businesses…. There’s a thought?
I talk with midwives and they tell me they are frightened, imagine going to work and being frightened, frightened because they’re so short-staffed. They are frightened that they’re going to harm a baby so the child never reaches their true potential, never has the life they should have, and even worse the baby dies. I’m talking about avoidable deaths. And women too, the thought of harming a women you are looking after is horrendous.
Rebecca protesting for more midwives
How can we expect people to work in this way?
One midwife said to me recently “I’m leaving before my PIN is taken off me”. Your PIN is your unique number which we all are given when we qualify. So, in other words, she left because of fear of being removed from the register. She was worried that something awful would happen on her shift, not because of her own wrongdoing, but because there aren’t enough midwives. It’s just not safe.
And the staffing numbers are getting worse, year on year … for the last few years we’ve been losing around 300 midwives per year, however the latest figures (reported last year/2022) are in fact worse and shows a loss of 677 midwives in a twelve month period. We cannot lose this many!
And if you think the solution is to train more midwives it’s not as easy as that. In order to increase the size of the workforce by just one full-time midwife, we need around 30 student midwives graduating. That’s because so many of midwives are leaving. It’s the leaky pipeline effect.
Now as well as midwives leaving because of safety concerns, there’s also a problem because we’re an aging workforce – Almost a third of midwives are in their 50’s and 60’s. These by definition are the most experienced with the most expertise, but inevitably they will all be retiring soon, so we could lose a third of our workforce in the next 5years. And this is the reality….if you lose 10 midwives each of them with 30 years experience then you lose 300 years of experience. That cannot be replaced with 10 newly qualified midwives. Fabulous as they’ll be but compare 10 to 300.
Also, if you keep on increasing the student numbers (which has been done recently), as we stand there are not enough lecturers to provide the teaching, not enough clinical placements to take them, the classrooms in universities aren’t even big enough! And not enough qualified midwife mentors or assessors to teach the students in the clinical area.
It’s catastrophic what is happening now and getting worse.
Maternity care is in crisis.
And too few midwives is a political decision. But it is the clinicians that get the blame when things go wrong, it’s the clinicians who end up in court, not the government.
It’s not an easy listen I know and I’m certainly no scaremonger, but it’s now come to such a crisis that we all have to face the current situation we are in regarding the care we are able to provide pregnant women.
Remember in midwifery we have two patients, not just one.
I’m sure many of you will have heard and read about the terrible scandals in maternity. Unnecessary deaths and harm to women and their babies. The impact is heart-breaking and devastating. Recently, there have been a number of very high-profile large investigations which have included many women and their babies. What was prominent about the Reviews was the catastrophic shortage of midwives as well as obstetricians and the lack of support for junior staff (midwives and obstetricians) and delays in appropriate review of care. All to do with the shortage of staffing.
So, Midwives (and doctors) haven’t all of a sudden become unkind, haven’t all of a sudden become uncaring, or incompetent. There just aren’t enough of them.
And here is why I believe moving this hospital to what looks like the New Royal’s site will not be of benefit to women, their families or the workforce
I believe keeping the hospital on the Crown Street site is a safe and viable option. Just recently the hospital has had their Care Quality Commission investigation. This is a routine assessment for all hospitals. The Report gives no indication that women are at risk due to the hospital being on Crown Street. The report does though identify poor staffing of midwives and obstetricians. Staffing will not improve if the hospital is moved.
What the hospital needs now is more midwives, more doctors, not closing down.
And something that always always needs saying, as many people I’m sure don’t know. Black women are nearly 4 times as likely to die in childbirth than white women. Asian women nearly twice as likely. Suicide in pregnancy is escalating, maternal deaths also on the increase. This is where the discussions need to be focused, this is where the energies of the Cheshire & Mersey ICB need to be focused.
These are the issues that need addressing, not how to close and move a hospital.
Everything I’ve said has all been the result of political decision making. Not a consequence of the NHS not working, the NHS is wonderful. It’s not broken it’s BEING broken. PURPOSELY.
We can’t let this cruel, nasty, evil government destroy lives. They are literally getting away with murder.
And its complicit ‘opposition’. They too are all literally getting away with murder.
Our campaign aim is clear. No closure. No privatisation. No cuts. No merger. Fully fund our hospital. And keep it on its Crown Street Site as a hospital dedicated to Women and Babies.
Greg Dropkin was one of the speakers at the recent wonderful Save Liverpool Women’s Hospital Demonstration on October 7th 2023
This is his speech. It was first published on labournet.net
The NHS is being privatised. To illustrate how, I’ll focus on two companies: Optum and EMIS Health. The Competition and Markets Authority has just authorised their merger, with Optum buying EMIS.
Optum is owned by the biggest US health insurance corporation, UnitedHealth, with an annual turnover of $324 billion. UnitedHealth has been fined over $1.1 billion for 374 violations of US laws. Optum paid Ohio $15m for overcharging the Workers Compensation Board for generic drugs. California and Arkansas are suing Optum and other Pharmacy Benefit Managers and pharmaceutical companies for wildly inflating the price of insulin.
Here, Optum has contracts with at least 19 Integrated Care Boards, and EMIS, formerly Egton Medical, has 30.
Cheshire and Merseyside ICB pays Optum for prescribing software, and EMIS for primary care hardware and software. EMIS manages patient electronic records in GP surgeries, community and hospital pharmacies. The merger means UnitedHealth subsidiaries will be active all across England, including in medicines management.
The US parent could also gain information derived from patients’ confidential medical records.
Optum and EMIS are accredited under an NHS England scheme to fast-track firms to develop integrated care. Contracts can be dished out to pre-approved companies. Optum’s accreditations include “sharing structured medications data for uses such as population health management, medications reconciliation, and decision support”. That’s despite Optum being sued for rigging the price of insulin, and overcharging for generic drugs.
Meanwhile, the notorious management consultancy PwC with a string of fines for accounting fraud, advises Cheshire & Merseyside on how and what to cut.
In their first year, Integrated Care Boards spent at least £6.4bn on private companies. NHS Trusts funded by ICBs have their own private contracts. In our region, around 27% of the ICB budget ends up with private firms, either directly or via the Trusts. North East and South East London are even worse.
How did we get here? Back in 2014, the Coalition government appointed Simon Stevens as NHS England Chief Executive. With no mandate from Parliament, NHS England introduced Accountable Care Systems based on a US funding model promoted by health insurance firms and consultancies including UnitedHealth and PwC. In 2018 it rebranded them as Integrated Care Systems. Last year, the Health and Care Act legalised what NHS England had already done. Systems have their own budgets, set using a Payment Scheme which can vary for different areas, providers, or types of patients. Private companies are consulted on the details.
The national health service is broken into 42 pieces. By destroying the national NHS economy, this could threaten national pay, terms and conditions, or staffing levels. Before Stevens was appointed to run the NHS, he was president of UnitedHealth Europe, CEO of its $30 billion Medicare business, and president of its global health businesses.
Before working for UnitedHealth, he advised Blair.
We all want the end of this vicious Tory government. But where is Labour? From Thatcher onwards, all governments have damaged the NHS. Most PFI hospital schemes, including the Royal Liverpool, were signed off under Labour. Blair’s government changed the rules on ownership of GP surgeries, enabling UnitedHealth and later Centene to take them over.
Independent Sector Treatment Centres were paid even if no treatment was given. Some clinical services went out to tender.
Canning Street
When the banks collapsed in 2008, Gordon Brown asked the US management consultancy McKinsey how to cut NHS spending. They said massive efficiency savings, dropping certain NHS treatments, and moving services out of hospital could save £15 – 20 billion per year. When Labour enacted their plan, the NHS funding crisis began.
Labour disowned Blair for invading Iraq, but never repudiated what Blair, Brown, Milburn, Reid, and Hewitt did to the NHS.
With rare exceptions, Labour accepts or embraces the current fragmented and part-privatised landscape. But it’s a disaster, and it’s not what we want.
We want the repeal of the Health and Care Act, and the NHS restored as a national health service. We want comprehensive, universal healthcare, publicly provided, publicly accountable, fully funded through progressive taxation, free at the point of need, with decisions on treatment taken on clinical grounds without regard to ability to pay.
That’s what we want, but whether we get it depends entirely on whether patients, healthworkers, and trade unions stand up to fight for it. I hope we’re ready.
Our NHS has been sliced up into Integrated Care Boards designed to deny care, close hospitals and pump money out of health care into private companies. Even the best-intentioned workers in these organisations cannot alter this fundamental design intention. You can’t make a silk purse out of a sow’s ear.
We, as campaigners in Cheshire and Merseyside, from different organisations and different parts of the area are determined to win back a publicly owned, publicly delivered, national health service for everyone. Every time an additional person is interested or involved we get a step closer to winning back our NHS.
The first step to save the NHS is to talk about what is really happening.
Public support for our stalls
Money spent on patient care repays itself rapidly and many times over. Poor healthcare cripples us and cripples the economy.
July’s 2023 ICB meeting, The people around the table listen to reports and decide on issues. The public sit and listen!
ICBs are not integrated, they are not improving care, and are making treatment harder to access. Millions are on the waiting list.
These are some of the questions we have sent to the NHS board meeting on September 28th. There are many more we could have sent.
Questions about Liverpool Women’s Hospital Appointment of a joint chief executive with Liverpool University Hospitals NHS Foundation Trust.
The problems patients and staff see at Liverpool Women’s are down to staffing and funding
We sent an earlier question soon after the announcement of the appointment of the joint Chief executive.
Question about the decision to share a Chief Executive with Liverpool University Hospitals Foundation Trust.
“What was the timeline for this decision and what role did the ICB play in it? Why was the women’s committee of the ICB not involved, or if it was, why were we told the opposite?
Please point us to the paper trail for making this decision.
Was the person spec for the original role also applied to the joint role?
Why was this not considered through ICB papers or meetings? Why was the public not consulted?
Why were representatives of the Campaign to Save Liverpool Women’s Hospital misled at a meeting that representatives of the board invited us to?
Can you provide reassurance that the well-documented difficulties at LUHFT are now so well under control that the management can take on responsibility for the largest women’s maternity hospital in the country without detriment to Cheshire and Merseyside’s women and babies?
(Page numbers reference relevant sections of the Board papers).
Page 86 Why is the continuity of care model still being recommended after Ockendon?
Page 144. When did the Women’s Committee meet? When is its next meeting? Where do we find minutes?
Page 172 What steps are being taken to ameliorate these risks?
Page 268 Maternity. Given the severity of maternity issues locally and nationally why is this section not more detailed?
Page 280 Liverpool Women’s Hospital is in Level 3 for financial concern yet cannot afford to provide full time consultant care at the Hospital. When will the ICB address the inadequacy of NHS funding for maternity as mentioned by Ockendon and other reports?
Page 327 Partnership board “including independent healthcare providers” Who are these organisations involved with the partnership board? What will their role be? Will they have voting rights?
Question about the money for Hospitals this year.
Re the expected CIPs (plus making good non-recurrent savings from last financial year).
From which areas of expenditure are you expecting trusts to make these “cost improvements”?
Final decisions within the set budget must rest with Trusts but in your planning for these targets, you must have scoped the possibilities of savings against increased risk to patients and staff.
How have you come to the conclusion that this level of CIPs is feasible? How have you ensured this is safely achievable?
Are staff numbers protected?
Are staff wages protected?
Is staff workload protected?
Is safety-critical equipment protected?
Will the number of patients be expected to fall?
Will certain treatments be limited?
How will these cuts be risk-assessed ?
Which vacancies will be filled?
Will hospitals already experiencing Opel 3 levels of difficulty even in the summer/early autumn still be expected to make cuts? (We hear from the health service journal that LUHFT ).
Questions about big US-based health corporations’ involvement in the ICB and the privacy of our most intimate records.
Board meeting
“The ICB holds a contract with Optum, concerning prescribing. In the US, Optum has been fined millions of dollars for violating laws on pricing of medicines. California charged Optum, other Pharmacy Benefit Managers and pharmaceutical companies with collaborating to rig the prices of Insulin. Optum is owned by UnitedHealth, the largest US health corporation, and is expected to merge with EMIS Health.
a) what due diligence did the Board conduct before awarding a contract to Optum?
b) how will a merger with EMIS affect prescribing policy?
c) how will the Board prevent UnitedHealth gaining access to individualpatient medical records?”
Questions about Covid.
PIcture credit to MJHIBLENART
Hello,
I would like to put the following to the forthcoming meeting of the ICB.
How is the ICB preparing for Covid this winter?
How will hospitals make preparations
given they are expected to make large cuts(CIPS) as described in the board paperwork.
given there are so many hospitals already on Opel level 3 in summer and early Autumn.
given Staff shortages and unfilled vacancies.
and given the number of NHS staff relying on food banks, suggesting weakened responses.
I refer you to the recent enquiry hearings which showed how badly the country was prepared for the first wave, with hospital infrastructure poor. SARS-CoV-2 frequently mutates and causes waves of infection and is to some extent seasonal. It is normal for The NHS to watch levels of Flu infections in the Southern Hemisphere Winter to plan for our Northern Hemisphere Winter infections. It would seem sensible to follow Covid levels similarly. Australia had a large and extended wave in its last winter, as reported in the BMJ 2023; Covid-19: Australia’s future policies will be evidence led after “profound impact” of latest wave, says minister.
How have you taken account of the Australian experience in your preparations for this winter?
I look forward to your response,
What is public, what is private?
Another campaigner has asked
I notice that agendas of C&M ICB meetings in public do not seem to include information about any private sessions that exclude press and public, and their agenda items – although other ICBs, such as West Yorkshire ICB, routinely do so.
Please would you let me know why this is? And does C&M ICB have any plans to include private sessions and their agenda items in the Agendas for future C&M ICB meetings?
This would be in the interest of public transparency, as it shows what topics the ICB is discussing and making decisions on in private, while still retaining confidentiality/privacy regarding the topics that are the subject of these private sessions.
Are you now going to tell the people of Cheshire and Merseyside the truth about what is being done to the NHS?
Given that:
the Cheshire and Merseyside integrated care system is set to carry out £58m CIPs (Cost Improvement Plans = cuts) this year, the various NHS Trusts and Foundation Trusts plan to achieve (i.e. cut) a further £331m in CIPs, and the ICS is expected to lose £350m funding in the next few years (according to the Review of Liverpool Clinical Services commissioned by the ICB); and that:
– the impact of these cuts will be to inflict further damage on people’s lives on top of a decade of cuts in access, beds, available staff; and that:
– the forty-two integrated care systems are modelled closely on the American accountable care system and their establishment dealt a death blow to the irreplaceable and effective (before deliberate cuts, fragmentation and privatisation) NATIONAL health service; and that:
– some Board members apparently took an oath to “first do no harm” (not to “first look after the bottom line” or “follow a plan devised in Minneapolis” or “allow patients’ data into the hands of a CIA operative”); and that:
– the public do not want a privatised system:
are you now going to tell the people of Cheshire and Merseyside the truth about what is being done to the NHS?
At the start of this post, we wrote “The first step to save the NHS is to talk about what is really happening.” Well, there are some more exciting things to do too including come to ur demonsration on 7th October in Liverpool:
For all our sisters,mothers, daughters and babies.