Questions to the ICB

Our NHS has been sliced up into Integrated Care Boards designed to deny care, close hospitals and pump money out of health care into private companies. Even the best-intentioned workers in these organisations cannot alter this fundamental design intention. You can’t make a silk purse out of a sow’s ear.
We, as campaigners in Cheshire and Merseyside, from different organisations and different parts of the area are determined to win back a publicly owned, publicly delivered, national health service for everyone. Every time an additional person is interested or involved we get a step closer to winning back our NHS.
The first step to save the NHS is to talk about what is really happening.

Money spent on patient care repays itself rapidly and many times over. Poor healthcare cripples us and cripples the economy.

ICBs are not integrated, they are not improving care, and are making treatment harder to access. Millions are on the waiting list.
These are some of the questions we have sent to the NHS board meeting on September 28th. There are many more we could have sent.
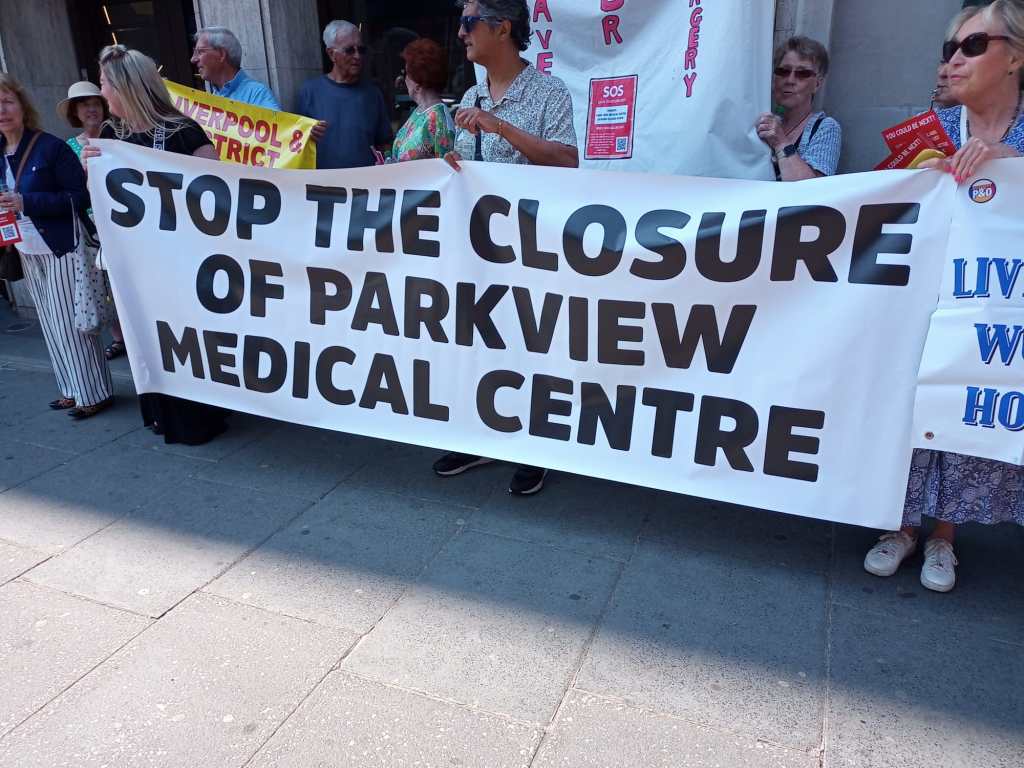
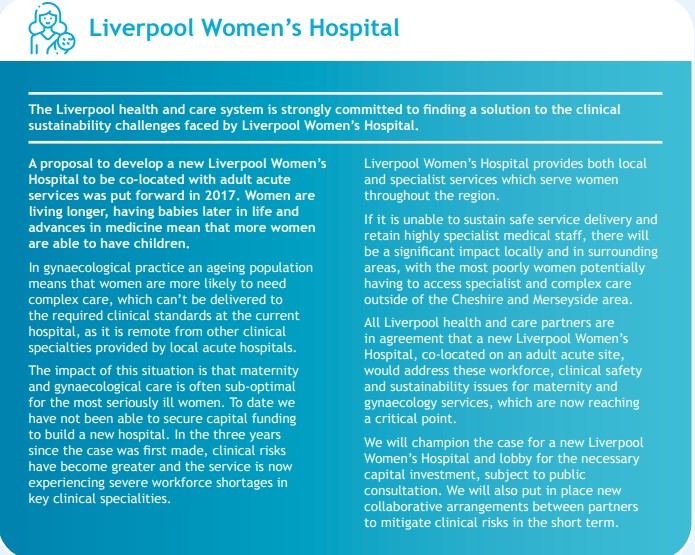
Questions about Liverpool Women’s Hospital Appointment of a joint chief executive with Liverpool University Hospitals NHS Foundation Trust.
We sent an earlier question soon after the announcement of the appointment of the joint Chief executive.
Question about the decision to share a Chief Executive with Liverpool University Hospitals Foundation Trust.
“What was the timeline for this decision and what role did the ICB play in it? Why was the women’s committee of the ICB not involved, or if it was, why were we told the opposite?
Please point us to the paper trail for making this decision.
Was the person spec for the original role also applied to the joint role?
Why was this not considered through ICB papers or meetings? Why was the public not consulted?
Why were representatives of the Campaign to Save Liverpool Women’s Hospital misled at a meeting that representatives of the board invited us to?
Can you provide reassurance that the well-documented difficulties at LUHFT are now so well under control that the management can take on responsibility for the largest women’s maternity hospital in the country without detriment to Cheshire and Merseyside’s women and babies?
(Page numbers reference relevant sections of the Board papers).
Page 86 Why is the continuity of care model still being recommended after Ockendon?
Page 144. When did the Women’s Committee meet? When is its next meeting? Where do we find minutes?
Page 172 What steps are being taken to ameliorate these risks?
Page 268 Maternity. Given the severity of maternity issues locally and nationally why is this section not more detailed?
Page 280 Liverpool Women’s Hospital is in Level 3 for financial concern yet cannot afford to provide full time consultant care at the Hospital. When will the ICB address the inadequacy of NHS funding for maternity as mentioned by Ockendon and other reports?
Page 327 Partnership board “including independent healthcare providers” Who are these organisations involved with the partnership board? What will their role be? Will they have voting rights?
Question about the money for Hospitals this year.
Re the expected CIPs (plus making good non-recurrent savings from last financial year).
From which areas of expenditure are you expecting trusts to make these “cost improvements”?
Final decisions within the set budget must rest with Trusts but in your planning for these targets, you must have scoped the possibilities of savings against increased risk to patients and staff.
How have you come to the conclusion that this level of CIPs is feasible? How have you ensured this is safely achievable?
Are staff numbers protected?
Are staff wages protected?
Is staff workload protected?
Is safety-critical equipment protected?
Will the number of patients be expected to fall?
Will certain treatments be limited?
How will these cuts be risk-assessed ?
Which vacancies will be filled?
Will hospitals already experiencing Opel 3 levels of difficulty even in the summer/early autumn still be expected to make cuts? (We hear from the health service journal that LUHFT ).
Questions about big US-based health corporations’ involvement in the ICB and the privacy of our most intimate records.
Board meeting
“The ICB holds a contract with Optum, concerning prescribing. In the US, Optum has been fined millions of dollars for violating laws on pricing of medicines. California charged Optum, other Pharmacy Benefit Managers and pharmaceutical companies with collaborating to rig the prices of Insulin. Optum is owned by UnitedHealth, the largest US health corporation, and is expected to merge with EMIS Health.
a) what due diligence did the Board conduct before awarding a contract to Optum?
b) how will a merger with EMIS affect prescribing policy?
c) how will the Board prevent UnitedHealth gaining access to individual patient medical records?”

Questions about Covid.

Hello,
I would like to put the following to the forthcoming meeting of the ICB.
How is the ICB preparing for Covid this winter?
How will hospitals make preparations
- given they are expected to make large cuts(CIPS) as described in the board paperwork.
- given there are so many hospitals already on Opel level 3 in summer and early Autumn.
- given Staff shortages and unfilled vacancies.
- and given the number of NHS staff relying on food banks, suggesting weakened responses.
I refer you to the recent enquiry hearings which showed how badly the country was prepared for the first wave, with hospital infrastructure poor. SARS-CoV-2 frequently mutates and causes waves of infection and is to some extent seasonal. It is normal for The NHS to watch levels of Flu infections in the Southern Hemisphere Winter to plan for our Northern Hemisphere Winter infections. It would seem sensible to follow Covid levels similarly. Australia had a large and extended wave in its last winter, as reported in the BMJ 2023; Covid-19: Australia’s future policies will be evidence led after “profound impact” of latest wave, says minister.
How have you taken account of the Australian experience in your preparations for this winter?
I look forward to your response,
What is public, what is private?
Another campaigner has asked
I notice that agendas of C&M ICB meetings in public do not seem to include information about any private sessions that exclude press and public, and their agenda items – although other ICBs, such as West Yorkshire ICB, routinely do so.
Please would you let me know why this is? And does C&M ICB have any plans to include private sessions and their agenda items in the Agendas for future C&M ICB meetings?
This would be in the interest of public transparency, as it shows what topics the ICB is discussing and making decisions on in private, while still retaining confidentiality/privacy regarding the topics that are the subject of these private sessions.
Are you now going to tell the people of Cheshire and Merseyside the truth about what is being done to the NHS?
Given that:
the Cheshire and Merseyside integrated care system is set to carry out £58m CIPs (Cost Improvement Plans = cuts) this year, the various NHS Trusts and Foundation Trusts plan to achieve (i.e. cut) a further £331m in CIPs, and the ICS is expected to lose £350m funding in the next few years (according to the Review of Liverpool Clinical Services commissioned by the ICB); and that:
– the impact of these cuts will be to inflict further damage on people’s lives on top of a decade of cuts in access, beds, available staff; and that:
– the forty-two integrated care systems are modelled closely on the American accountable care system and their establishment dealt a death blow to the irreplaceable and effective (before deliberate cuts, fragmentation and privatisation) NATIONAL health service; and that:
– some Board members apparently took an oath to “first do no harm” (not to “first look after the bottom line” or “follow a plan devised in Minneapolis” or “allow patients’ data into the hands of a CIA operative”); and that:
– the public do not want a privatised system:
are you now going to tell the people of Cheshire and Merseyside the truth about what is being done to the NHS?
At the start of this post, we wrote “The first step to save the NHS is to talk about what is really happening.” Well, there are some more exciting things to do too including come to ur demonsration on 7th October in Liverpool: