Privatisation is part and parcel of the Maternity Review and the Governments plans for the NHS. Mersyside and Cheshire are one of the first areas to start it.
In the previous post we wrote about the need for NHS based home births but the “One to One” name locally is associated with a private for profit company/ companies providing NHS funded maternity care.
What’s the problem with private providers getting mixed up with the idea of choice in childbirth?
At each stage of pregnancy, Midwife support links to other potential back up providers like ambulance and hospitals.. One to one midwives, either private or NHS, rely on the NHS for back up. 50% of first time mothers giving birth in the home have to be transferred to hospital.
This privatized provision is part and parcel of current provision for the NHS. Clinical Commissioning Groups decide which organisations they will pay to provide services. One to One company is commissioned in Wirral and in Liverpool and maybe more places.
Merseyside and Cheshire are a vanguard area for the Maternity Review. The sweet words say “Pregnant women living within the pioneer areas will be offered a personal budget and will be able to use it to make choices for each of three stages of the pathway – antenatal, intrapartum and postnatal care..This means a woman would have a wider choice of who provides the maternity care she would prefer, such as a birthing pool, specialisation in teenage, older, or first time mothers, or a provider with a good reputation for breastfeeding support.NHS England and other partners will work with the pioneers to develop and test new approaches which can then be rolled out nationally.” england.nhs.uk/healthbudgets/2016/05/18/greater-choice-of-care
The reality is somewhat different. We already have all of the above provided and at international levels at Liverpool Women’s Hospital, including “a birthing pool, specialisation in teenage, older, or first time mothers, or a provider with a good reputation for breastfeeding support.” Liverpool Women’s Hospital is seind in the country for breast feeding support.
There are serious issues reported with the private company delivering midwifery care on Merseyside, in this case in Wirral.
We think that the midwives who work for the company are as well intentioned as those in the NHS. We know that the pressure of work in the NHS is very high and there is a good reason to try an alternative model of work, but there are problems. Other midwives might have struggled to get a position in the NHS or had other good reasons to work for One to One but this does not overcome the problem that the model is flawed..
There have been problems with the training of midwives about diabetes and epilepsy in pregnancy. The following is a response to a freedom of information request to the CCG
We quote it exactly so we cannot be accused of misreporting. Please take time to read this.
“The service did not always measure safety issues against quality targets and so could not be sure the processes were protecting women and babies from abuse and avoidable harm were as effective as possible... Protocols were needed to ensure girls aged 18 and under were protected if they contacted the service. The service had a named lead safeguarding midwife whose duties were outlined in the One to One adult safe guarding policy; however, dealing with potential child protection issues were not addressed. Information provided did not provide assurance that the service dealt with child protection issues appropriately. For example, the One to One referral pathway identified that only young women aged 14 years and over were eligible for the service, but staff were not prompted to involve the criminal justice system if a 13-year-old became known to them. Neither were staff prompted to make vulnerable young people enquiries for those aged between 14 and 18 years old. The service planned to increase the number of safeguarding supervisors with training by the NSPCC by April 2016
The One to One safeguarding adult’s policy (version2) 2014 was not specifically relevant to the community based services; however, the policy prompted midwives to refer to and follow the relevant local authority safeguarding policy.
The safeguarding policy did not reference actions midwives should take if they were aware the female genital mutilation had occurred.
We were informed there was a longstanding relationship both with the safeguarding team at the Local Acute Trusts, the CCG on the Wirral and neighbouring CCG areas. Safeguarding referrals were monitored through reporting arrangements with each CCG using dashboards.
It was reported that the named midwife for safeguarding had regular meetings with the designated nurse for safeguarding at Wirral/West Cheshire/Warrington CCG to ensure all legal and contractual requirements were met. This was monitored through contractual obligations with lead CCGs.
The ‘Safeguarding Level 3 training Action Plan’ provided at the time of the inspection indicated 80% of staff had completed safeguarding level three training. This was worse than the service’s target of 95%. The action plan stated the target for achieving 95% compliance was April 2016. Further training had been planned to reach the compliance target.
Another report, quoting from the CQC Report (27 June 2016) said
“At an earlier inspection in April 2015 “we were not given the assurance that risk was being managed effectively across the organisation to provide a safe environment for high risk pregnancies. At that inspection we also found no evidence of joint pathways in place with local providers and agreed processes for flagging up or considering additional needs of the mother were not in place. We asked the provider to make improvements in these areas.”
The CQC returned on 30 Nov and 1 Dec 2015. “We found that incidents were not being reported to CQC under the statutory notifications’ regulation. The incidents the staff were required to report to CQC was limited to “serious incidents which has potential to threaten registration status”. The clinical incident policy did not require staff to report clinical incidents to CQC. Regulation 18 of the CQC (Registration) Regulations 2009 requires providers to notify CQC of certain defined incidents. This would include incidents of patients experiencing prolonged pain or prolonged psychological harm or certain types of injury to a service user.”
“Two serious incidents were reported to the Care Quality Commission between April 2015 and December 2015. This involved one intrauterine death, one intrapartum death. One neonatal death which involved joint care with an NHS trust was also reported.
“Our records indicated that the CCG informed the Care Quality Commission about two of these occurrences. We had to seek additional information from the One to One services about all incidents. This meant the service was not fulfilling their obligation to provide CQC with notifications of incidents required under the Act.”(our emphasis)
“Concerns remained about how well high risk pregnancies were monitored during pregnancy because staff stated they had not received specialist training to support women with underlying conditions such as epilepsy and diabetes. Concerns were also raised about action taken for women who may develop unforeseen complications who then refused to seek medical intervention and/or hospital support when midwives identified that this was needed.”
“Risks within the organization were identified and included safeguarding training rates for midwives, potential gaps in the handover process between midwives when the lead midwife was unavailable and; women who chose to deviate from NICE guidance who also had complex needs with a risk of overall poor outcomes. A gap in integrated working with other providers was also identified as a risk.”
“The service did not always measure safety issues against quality targets and so could not be sure the processes were protecting women and babies from abuse and avoidable harm were as effective as possible. Care pathway risk assessments for antenatal care and protocols for dealing with emergencies were unclear and did not provide a firm basis on which to support home births for high risk pregnancies. Protocols were needed to ensure girls aged 18 and under were protected if they contacted the service.”
“The service accepted women with low and high risk needs, however specialist midwives for epilepsy, diabetes, mental health or substance misuse were not employed and women were not automatically referred to NHS trust specialist services.”
“Policies did not always promote the safest response to the results of risk assessments. For example, the One to One ‘Discharge of care practice point 2011’ stated ‘Antenatal transfer of care should only be initiated by the woman. One to One will provide midwifery care for all women regardless of risk.’ The policy did not provide additional guidance for staff if a woman would not transfer when the level of risk included a high likelihood of injury or mortality.”
“High court proceedings underway against this provider could result in insolvency”. http://www.liverpoolccg.nhs.uk/media/1742/gb-agenda-14-june-2016.pdf
We have invited One to One to talk to us. That invitation is still open.
Privatisation of the delivery of babies is a very bad idea. If it is part of moving away from Consultant led hospitals in this area its a very bad idea indeed.
Home biths are not a cheap option. They are an addition to the main service..Save Liverpool Women’s Hospital





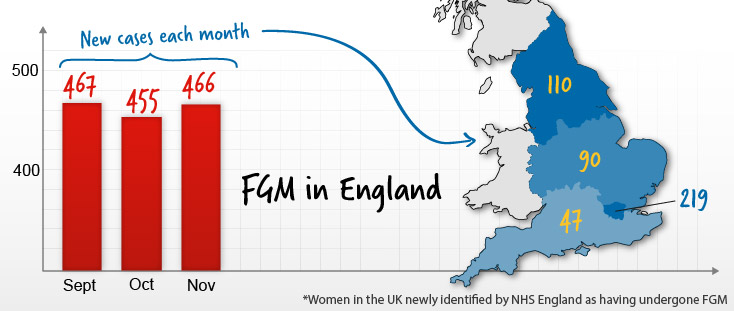 The hospital is located in an ethnically diverse part of town. Some of the women in this community who would need to access a FGM clinic may not be used to using buses to get perhaps to Aintree.. Liverpool Women’s Hospital is well trusted in the local community., and local women safe and respected going there.There could be could have language barriers that make it difficult to just hop on a bus to get across town. If the Liverpool Women’s Hospital is closed and the FGM clinic moves across town, there is the potential issue that women who need the service face a load more barriers to getting it. Basically, local women will suffer.
The hospital is located in an ethnically diverse part of town. Some of the women in this community who would need to access a FGM clinic may not be used to using buses to get perhaps to Aintree.. Liverpool Women’s Hospital is well trusted in the local community., and local women safe and respected going there.There could be could have language barriers that make it difficult to just hop on a bus to get across town. If the Liverpool Women’s Hospital is closed and the FGM clinic moves across town, there is the potential issue that women who need the service face a load more barriers to getting it. Basically, local women will suffer.