

Save Liverpool Women’s Hospital Campaign Group’s International Women’s Day Celebrations
8th March 2022
The following is the transcript from Dr Rebecca Smyth’s talk: ‘The Gender Data Gap’
Hello everyone,
Firstly, Happy IWD to you all!
Each year the IWD organisation identify a theme.
And this year the campaign theme is: BreakTheBias
Here is a quote from their website (IWD organisation), this is what they say:
Imagine
A gender-equal world.
A world free of bias, stereotypes, and discrimination.
A world that is diverse, equitable, and inclusive.
A world where difference is valued and celebrated.
Together we can forge women’s equality.
Collectively we can all BreakTheBias.
(https://www.internationalwomensday.com/theme March 2022)
I am going to talk for a few minutes about women and health, with a particular focus on bias, given this year’s theme. As we all know your sex has a significant impact on your health, so let’s see if we can start to better recognise this bias and think of ways to BreakTheBias.
I think we all agree that roughly half the world is inhabited by women (49.6%), half by men (50.4%) (I’m excluding animals and plants here by the way), based on 2020 figures. However, that’s where the fairness of the divide ends.

In my talk I’m going to focus on the inequalities there are in access to healthcare and healthcare outcomes for women. I’m wanting to identify some of the bias that is present.
But before I do, I think we need to consider and acknowledge where the ‘evidence’ comes from / where our ‘knowledge’, where our ‘understanding’ comes from. Because recognising this goes some way to BreakTheBias, or we could call it unfairness or we should actually call it discrimination.
Most of our ‘knowledge’ about health, some would actually say pretty much everything we know uses data, and it is this data that is male-biased in other words the data favours men and does not reflect the true world we live in. So, our decision-making, healthcare treatments for example are based on data gathered from men and this is known as ‘the gender data gap.’ It is where a “one size fits all” approach has been used, however it has left gaps in our understanding of the experiences of women because it is male-biased. Women have basically been excluded. So, the upshot is that most of what we understand is skewed in the favour of men. It’s a male-default world we live and we need to Break this Bias.
If I can give you some examples. The one many of you will know and which is perhaps a little light-hearted, nevertheless annoying and one I think all of us can relate to is room temperature. I’m sure we know all about room temperature at home. And there is ample evidence that office environments are tuned to male biology. Air conditioning is often set according to a 1960s formula based on the metabolism of a 40-year-old man who weighs 11st. Previous studies have suggested that the average woman is most comfortable at about 25C, 3C higher than for men. Because women generally have a lower metabolic rate than men because of their body composition so they prefer warmer rooms and need less air conditioning. (Koch; National Geographic 2015). However, this has still not been corrected in many offices (or homes!).
Another light-hearted one… mobile phones. Like the standard piano keyboard, smartphones have been designed for male hands and therefore may be affecting women’s health adversely. It is a relatively new field of study, but the research that does exist is not positive. Within the studies, women were significantly under-represented and the vast majority of studies do not break down the data by sex. The few that did report a statistically significant difference in the impact of phone size on women’s hand and arm health as well as physical comfort (Kwon 2016). Speech-recognition software is trained on recordings of male voices: Google’s version is 70% more likely to understand men (Criado Perez 2019).
Here’s another one for you demonstrating the gender data gap: we all know that women even when in paid work still do the majority of the housework (McNunn 2018, UCL Epidemiology & Health Care). Yet it is documented that fitness monitors underestimate steps during housework by up to 74% and calories burned during housework by as much as 34% (Criado Perez 2019).
So why should we think these are just light-hearted examples, why should we not consider that these types of bias play out in much more important aspects of our lives, health, work, politics and political decision-making. The ‘gender data gap’ is everywhere. Let’s Break this Bias.
Regarding health, let’s talk about heart attacks.
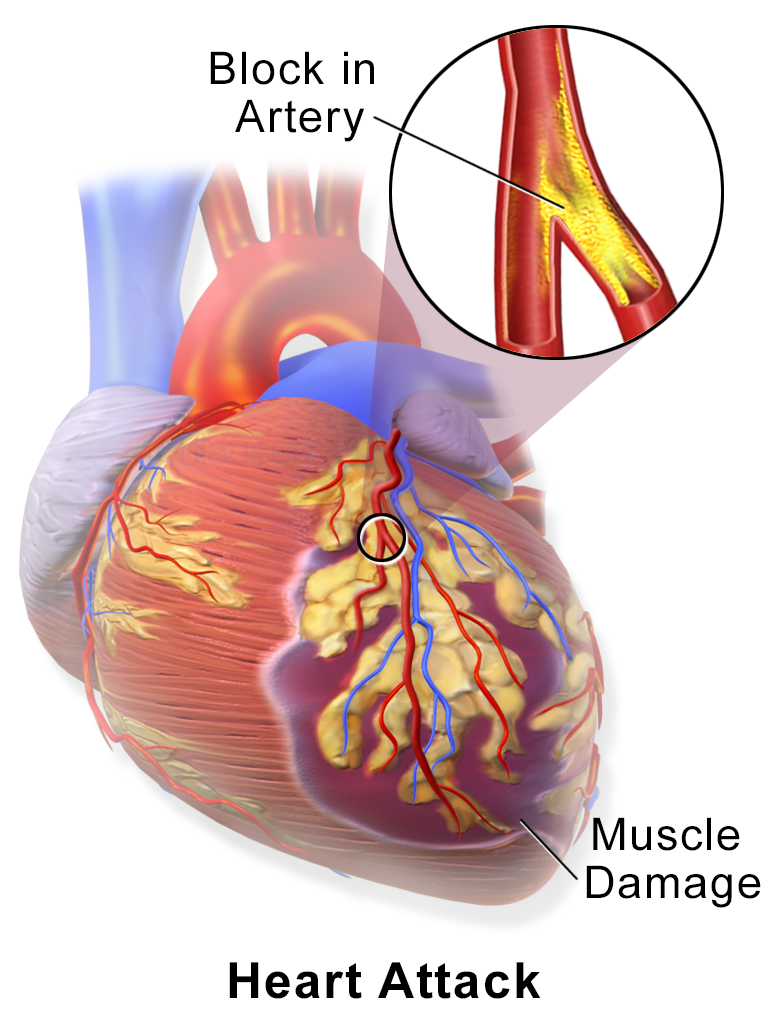
Early diagnosis of a heart attack is essential for treatment and survival. Research by the British Heart Foundation (BHF) has shown that women having a heart attack are up to 50% more likely than men to receive the wrong initial diagnosis. Women are also less likely to get a pre-hospital ECG also. And someone who has an incorrect initial diagnosis of heart attack has a 70% higher risk of death after 30 days compared to someone who receives the correct diagnosis straightaway. So, this is serious.
This is because of how we have been informed (and by we, I mean everyone, healthcare workers too) as to what the signs and symptoms of a heart attack are. That’s because we are basing our knowledge solely on the male experience, on what male symptoms are. In fact, over a ten-year period, more than 8,200 women died needlessly following a heart attack. They could have been saved if they had received the same quality of care as men. The BHF call this ‘Bias and Biology’. Here is a quote from a woman who suffered a heart attack. She says… “Doctors thought my symptoms were due to asthma, stress and anxiety at a time when I was changing jobs. But on holiday I had a heart attack and the very next morning I was sent for heart bypass surgery” (Simone Telford 2022). We need to Break this Bias.
Some symptoms of a heart attack do differ between the sexes (British Heart Foundation May 2022). A study by the BHF (May 2022) found more women had pain that radiated to their jaw or back and women were also more likely to experience nausea in addition to chest pain (33 per cent vs 19 per cent). Whereas, the less typical symptoms, such as epigastric pain (heartburn), back pain, or pain that was burning, stabbing or similar to that of indigestion, were more common in men than women (41 per cent in men vs 23 per cent in women). Important to know that women tend to wait longer before calling 999 after first experiencing heart attack symptoms. And we know any delay can dramatically reduce your chance of survival. Additionally, heart attacks are often seen as a male health issue, but more women die from coronary heart disease than breast cancer in the UK. So we really need to Break this Bias, because this misconception is leading to avoidable suffering and loss of life (Pearson, BHF Associate Medical Director 2022). (An interesting video for anyone concerned about heart attacks in women from NHS Scotland here)
Let’s talk about women in research…
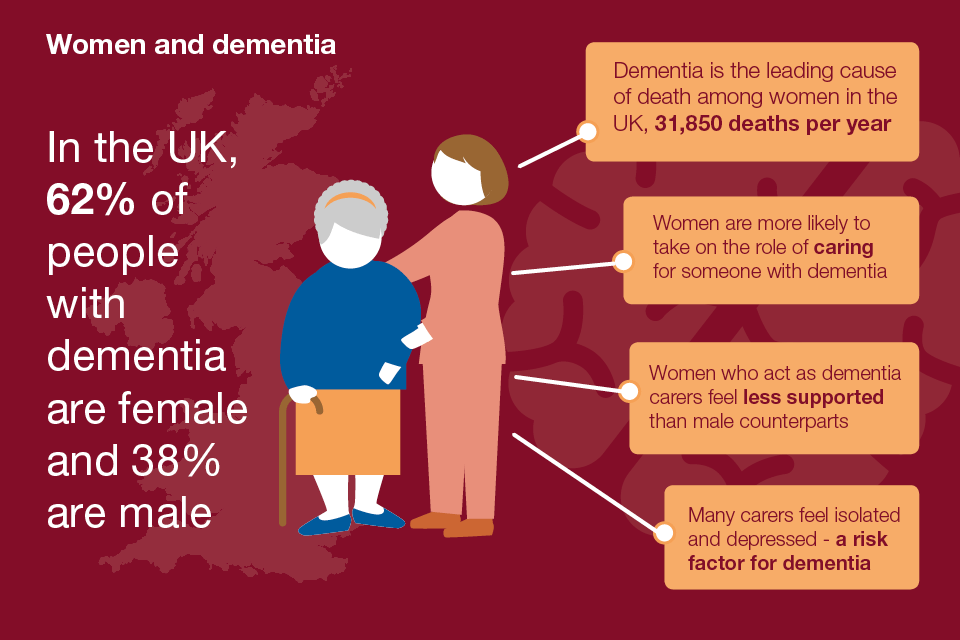
Think of another example, Alzheimer’s. In the UK Alzheimer’s disease is almost twice as common in women compared to men. Now, why is it more common in women than men? Well for a long-time clinicians and researchers put it down to the fact that women live longer than men, and didn’t explore it any further. It is only more recently that researchers have begun looking past this assumption, and early discoveries indicate that the impact of biological underpinnings may contribute to the underlying brain changes. Evidence demonstrates that women with dementia have fewer visits to the GP, receive less health monitoring and take more potentially harmful medication than men with dementia, new UCL research reveals (Dayantis 2016). So, for many years bias was present, we need to Break this Bias.
The under-representation of women in clinical trials stems from the long-held assumption that the male perspective represents the norm. For those of you with clinical interest, you will know that medical education textbooks typically default to the male in case studies and anatomical drawings, while women are represented only in matters specific to reproductive biology (Liu 2016).
Differences in pharmacokinetics of drugs between the sexes can be related to body composition and size (Wizemann T, Pardue 2001). Women typically have a lower body weight than men, so when taking the same dose of a drug, results in a higher level of the drug (Parekh 2011, Wizemann 2001). That’s why we see an increase in adverse drug reactions in women. In fact, data suggests women experience adverse drug reactions nearly twice as often as men (Zucker 2020)

However, women have been excluded from pharmaceutical research for many reasons (Yakerson 2019). Now we can’t ignore the thalidomide tragedy of the 1960s which prompted a protectionary ban on pregnant women and women of child-bearing age from participating in clinical trials. Other obstructions are the perceived complexity and higher costs of studies if women are included, women’s unwillingness to participate, and the pervasive treatment of the male body as the norm (Yakerson 2019). They also viewed women as confounding and more expensive to research because of their fluctuating hormone levels (Wizeman 2001). Well, all I can say is we’d be extinct without our ‘fluctuating hormone levels!
It was only in 1993 (29 years ago) that the landmark US National Institutes of Health (NIH) Revitalization Act changed the model from excluding women to recommending their inclusion in phase III clinical trials (Zucker 2020). So improvements are being made however, the International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use (ICH brings together regulatory authorities and the pharmaceutical industry) has not recognised the need for specific, standalone guidelines on the inclusion of women, continuing to refer to women as a special subgroup to be considered when appropriate (https://admin.ich.org/sites/default/files/2019-04/ICH_Women_Revised_2009.pdf). We need to Break this Bias.
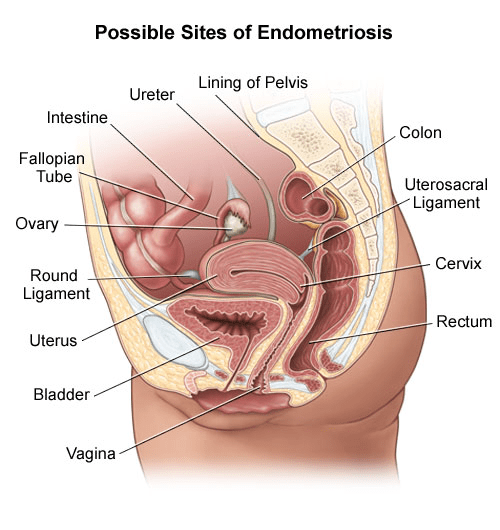
Less than 2.5% of publicly funded research is dedicated solely to reproductive health (“UK Health Research Analysis 2014 (UK Clinical Research Collaboration, 2015) http://www.hrcsonline.net/pages/uk-health-research-analysis-2014”), despite the fact that one in three women in the UK (34%) will suffer from a reproductive or gynaecological health problem (https://www.gov.uk/government/news/survey-reveals-women-experience-severe-reproductive-health-issues 2018). Endometriosis affects one in 10 women, which means it is as common as diabetes in women. The proportion of funding that goes into diabetes far exceeds the levels of funding that goes into endometriosis.
There is five times more research into erectile dysfunction, which affects 19% of men, than into premenstrual syndrome, which affects 90% of women (Slawson 2019, https://www.theguardian.com/education/2019/dec/18/women-have-been-woefully-neglected-does-medical-science-have-a-gender-problem). I’ll leave it there. Let’s Break this Bias.
If I give an example of pregnant women in Covid research trials: The disparity in trial inclusion has been exacerbated in the covid-19 pandemic, in fact, pregnant women initially were not included in covid-19 vaccine trials. A recent review reported that of 927 trials related to covid-19, 52% explicitly excluded pregnancy, 46% did not mention pregnancy, and only 1.7% specifically included pregnancy (Smith 2020)
This initial exclusion evidently impacted the very slow uptake of the vaccine in pregnant women. In Dec 2021, the RCM and RCOG emphasised the urgency for pregnant women to receive the vaccine, that’s because at that time three-quarters of all ICU patients with Covid-19 were pregnant women. That’s the consequence of not Breaking this Bias. The default position should be to investigate and treat pregnant and breastfeeding women in the same way as non-pregnant women unless there are clear reasons not to (Knight 2019).
Time has not allowed, but I think we should return to this another time about the appalling under-representation of minority ethnic groups in research as well as women from deprived areas / lower socio-economic groups (Redwood and Gill 2013). Lots more can be said about these issues.
I’ll just end on, if we are going to achieve any kind of equality, then it is essential we have equal participation and leadership of women in political and public life. However, data shows that women are underrepresented at all levels of decision-making worldwide, and achieving equality in political life is far off. In our government, 35% of MPs in the House of Commons are currently women, and this, this is an all-time high. And in the House of Lords, it is 28% and around just 36% of local authority councillors in England are women.
If we are going to get anywhere with any of this we need to BreakTheBias
Rebecca Smyth 08/03/22
Endometriosis link <a href=”http://”>here
