
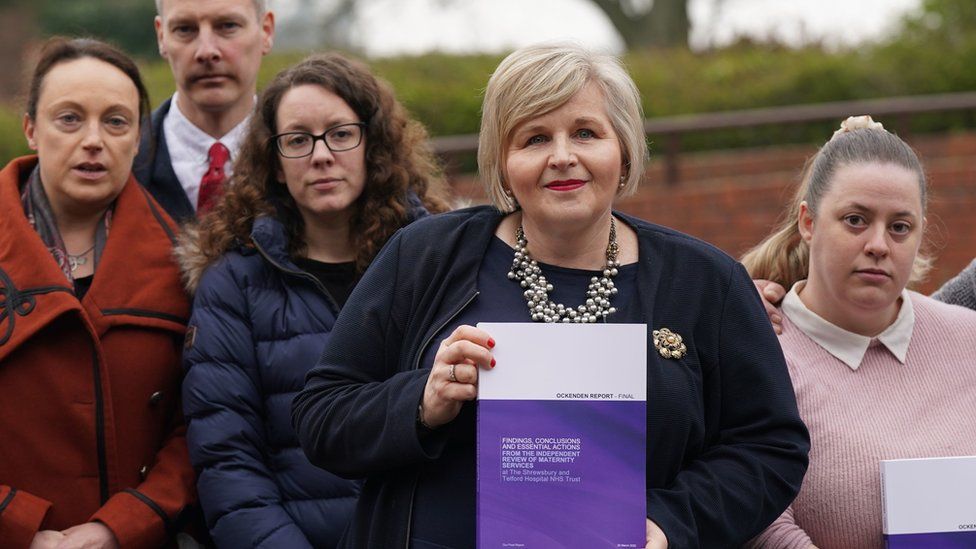
It is with great sadness that we read the findings from The Ockenden Review and we add our thanks to the families who fought so hard to bring their experiences to public attention. As midwives and campaigners for safe and compassionate maternity care we have a duty to reflect on the findings of this report and our thoughts are with the women, their families and staff working at The Shrewsbury and Telford Hospital NHS Trust. The Lancet commented that;
“The report found that around 200 babies and nine mothers would or might have survived if the trust had provided better care. The Royal College of Obstetricians and Gynaecologists (RCOG) called it a “dark day”. Criminal charges might still be brought against the Trust and individuals.”
Donna Ockendon gave great credit to the parents whose campaigning instigated the report;
“The work contained in this final report and the first report of the Independent Review of Maternity Services at the Shrewsbury and Telford Hospital NHS Trust, came about from the exceptional efforts of parents Rhiannon Davies, Richard Stanton, and Kayleigh and Colin Griffiths, whose daughters died as a result of the care they received at the Trust.
The deaths of Rhiannon and Richard’s daughter Kate in 2009, and Kayleigh and Colin’s daughter Pippa in 2016 were both avoidable. Owing to their unshakeable commitment to ensure the precious lives of their babies were not lost in vain, this review has implementation of meaningful change, not only in maternity services at The Shrewsbury and Telford Hospital NHS Trust – but also across England. As we publish this final report, we want to acknowledge and pay tribute to Rhiannon, Richard, Kayleigh and Colin.“
Shrewsbury is not alone. There have been other maternity scandals in Morecombe Bay, Essex and Nottingham.
The crisis in maternity staffing in 2022 is worse than the period covered by this report. Many hospitals did manage against the odds to avoid some of the damage done in Shrewsbury. Shewsbury’s managers and senior clinicians have serious questions to answer. The context does not excuse their actions but it is crucial to understanding what was happening.
Understanding and appreciating the context in which these failures happened is a vital step in working towards any type of prevention. What is prominent throughout the review is the catastrophic shortages of midwives, medical staff and other maternity healthcare workers and the impact these shortages have had on care. For many years we have known of these critical shortages and the tragic damage this would cause. Now, sadly, we are seeing it.
With this shortage comes poor supervision and training of staff, in particular preceptorship programmes for newly qualified midwives (NQM). Without enough qualified midwives, it is impossible to provide supernumerary status with protected learning time for NQMs. This is crucial if we want to grow a competent and confident workforce.
Donna Ockendon says;
“It is absolutely clear that there is an urgent need for a robust and funded maternity-wide workforce plan, starting right now, without delay and continuing over multiple years. This has already been highlighted on a number of occasions but is essential to address the present and future requirements for midwives, obstetricians, anaesthetists, neonatal teams and associated staff working in and around maternity services. Without this maternity services cannot provide safe and effective care for women and babies. In addition, this workforce plan must also focus on significantly reducing the attrition of midwives and doctors since increases in workforce numbers are of limited use if those already within the maternity workforce continue to leave. Only with a robustly funded, well-staffed and trained workforce will we be able to ensure delivery of safe, and compassionate, maternity care locally and across England.“

Yet, how can a maternity service be safe and compassionate if there aren’t enough staff? How can staff give women their time, time to sit and talk, time to listen. It is impossible. It cannot be done. As a consequence, women will not be provided with the safe and compassionate care they so justly deserve, not because staff don’t care, but because there simply aren’t enough of them.
In July 2021 the report on the Safety of Maternity Services from the Parliamentary cross-party Health and Social Care Committee said;
“With 8 out of 10 midwives reporting that they did not have enough staff on their shift to provide a safe service, it is clear that urgent action is needed to address staffing shortfalls in maternity services. Evidence submitted to our inquiry estimates that as a minimum, there need to be 496 more obstetricians and 1,932 more midwives. While we welcome the recent increase in funding for the maternity workforce, when the staffing requirements of the wider maternity team are taken into account–including anaesthetists to provide timely pain relief which is a key component of safe and personalised care – a further funding commitment from NHS England and Improvement and the Department will be required to deliver the safe staffing levels expectant mothers should receive.”
“We recommend that the budget for maternity services be increased by £200–350m per annum with immediate effect. This funding increase should be kept under close review as more precise modelling is carried out on the obstetric workforce and as Trusts continue to undertake regular safe staffing reviews of midwifery workforce levels.“.
Despite this recommended additional funding for maternity, the government produced only half of what the committee said was needed. The Government did not even respect a parliamentary committee.
A whole year has been lost that could have stopped the current situation from developing. That funding has still not been provided.
Donna Ockendon reported on maternal deaths, baby deaths and the injury to some of the babies. She wrote this of the Cerebral Palsy cases;
“All of the families in this group self-reported to the review. The diagnosis of cerebral palsy was often made some years following their maternity episode. On reviewing the medical records, where it was found that the neonatologists at the Trust had recorded a diagnosis of HIE [(hypoxic-ischaemic encephalopathy] in the early neonatal period, a small proportion of families were subsequently transferred to the HIE incident category. From the remaining cases of cerebral palsy, more than 40 per cent were identified to have significant or major concerns in maternity care which might have resulted in a different outcome.”
Mistakes will be made in any field of medicine, though few with such catastrophic results as mistakes, or carelessness, in maternity care. Lessons must be learned from every incident and changes implemented quickly. This failed disastrously in Shrewsbury and the fault is not with the midwives (though significant mistakes were made ), but with the hospital management.
The government has made and is still making appalling decisions in funding and managing the NHS and particularly in maternity. A quick check on MumsNet today found a mother refused an induction despite her concern about her near term baby’s reduced movements. We are told to Count the kicks yet even today after Ockendon has reported, women are not always heeded.
The bureaucracy of the NHS also bears responsibility, if only for failing to describe publicly the damages from Government policies including; the shortages of funds for the NHS, bad workforce planning, the closure of beds and maternity units, not calling out the disaster of the “internal market” and for “managing” the news around incidents. We saw a pretence that all was well, whilst embarking on expensive new initiatives, like Continuity of Carer, without adequate funding and thereby driving out still more midwives. A background of bullying and silencing staff is also important. The number of midwives quitting because they do not feel that the system is safe surely should have been a warning to all.
Donna Ockendon notes
“The key themes identified requiring improvement within maternity services at the Trust were:
• The poor quality of incident investigations
• Poor complaints handling
• Local concerns with statutory supervision of midwifery investigations
• Concerns with clinical guidelines and clinical audit
…the review team has identified the following concerns regarding governance in
maternity services at the Trust:
a) Incidents that should have triggered a Serious Incident investigation were inappropriately
downgraded to a local investigation methodology known as a High Risk Case Review (HRCR),
apparently to avoid external scrutiny.
b) When serious incident investigations were conducted many were of poor quality.
c) There was a lack of learning and missed opportunities to improve safety.
d) There was a lack of oversight of serious incidents by the Trust’s commissioners.
e) There were repeated persistent failings in some incident investigations as late as 2018-2019.
4.8 The review team has found a concerning and repeated culture at the Trust of not declaring adverse
outcomes as an SI in line with the national framework. Instead, they were inappropriately downgraded
and investigated by what the Trust termed a High Risk Case Review (HRCR). This method of investigating
incidents, created by the Trust, was less robust, varied considerably in quality and lacked the rigour and
transparency of an SI investigation. Notably, HRCRs were not reported to NHS England, the Clinical
Commissioning Groups (CCGs) or the Trust Board, and therefore avoided external scrutiny.“
The Review also importantly recognises the damming consequence of Cumberlege’s National Maternity Review and the Midwifery Continuity of Carer model. With such poor staffing, such a programme not only cannot but should not have been implemented. We welcome The Reviews Essential Action for the suspension of this provision unless Trusts can demonstrate safe staffing levels on all shifts. The Review acknowledges the unprecedented pressures that the model places on services, services already under significant strain and the impact of which compromised the safety of pregnant women and their babies. We support the need for robust evidence to assess if it is a model fit for future maternity care. Currently, that evidence does not exist.
What is evident from The Review is the harm mothers and babies suffered from what appears to be withholding the use of caesarean sections. We will watch with caution the end of total caesarean section percentages as a metric for maternity services, as potentially we could see rates escalate and we urge continued careful monitoring.
Apparent in The Review, is the fear staff had to speak out about their concerns. There can be no transparency, and no openness to change if free speech is not allowed.
Save Liverpool Women’s Hospital Campaign has been working since 2016 to
- Expose the flaws in the funding and structure of maternity provision and
2. To support all who continue to work in maternity despite the odds.
3. To demand excellent maternity care for all, (including migrant women, who face dreadful charges for maternity care).
4. To fight for women’s healthcare.
5. To protect our hospital, Liverpool Women’s Hospital, on its Crown Street site.
6. To campaign for the NHS to remain free at the point of need, funded by the government, providing universal and comprehensive care, publicly owned and publicly delivered.

A publicly provided, well funded, universal maternity service, free at the point of need is essential. There is no solution to the problems the NHS faces to be found in privatising it. Cuts, shortages, coverups of shortages, and bullying, cannot keep our mothers, sisters, daughters, friends and lovers and every precious baby, safe.
The figures for maternal deaths in the US privatised model quoted by The Commonwealth Fund, prove this:
“Key Findings: The U.S. has the highest maternal mortality rate among developed countries. Obstetrician-gynecologists (ob-gyns) are overrepresented in its maternity care workforce relative to midwives, and there is an overall shortage of maternity care providers (both ob-gyns and midwives) relative to births. In most other countries, midwives outnumber ob-gyns by severalfold, and primary care plays a central role in the health system. Although a large share of its maternal deaths occur postbirth, the U.S. is the only country not to guarantee access to provider home visits or paid parental leave in the postpartum period.
Conclusion: The U.S. has a relative undersupply of maternity care providers, especially midwives, and lacks comprehensive postpartum supports.“

Women were not heard or heeded in many of these tragic events, indeed some were themselves blamed by the hospital.
Importantly, we must not forget the blame for all of these lies squarely at the feet of the government. Continued cuts year on year are destroying maternity services and the NHS as a whole. Allowing chronic staff shortages, poor staff satisfaction, high staff attrition rates, and unsafe working conditions are all political choices made by this government. Now we see mothers and babies dying. These are all political choices.

Women have a right to excellent maternity services. It is the government’s responsibility to provide this. This is the contract between citizens and the government Women must have the right to choose how they have their baby. Women are entitled to have the best advice on these choices. Women have the right to expect emergency backup when this is required. Women have the right to be both heard and heeded, especially when things start to go wrong. Women have the right to be heard and to participate in all reviews of serious incidents. Ockendon will strengthen these rights.
There is a thread in the media saying that natural births were somehow to blame. There is nothing in Ockendon to say this. Ockendon does say that poor monitoring, failures to intervene early, failure to use cesarean sections when urgently needed, and failure to listen to mothers, were all faults.
.

Midwives are a highly valued profession. Midwives can make mistakes, of course, but the faults described in Ockendon do not blame midwives as a profession. A service with a good supply of well trained, and well respected (and well paid) midwives, helps save lives.
The Royal College of Obstetrics and Gynaecology reported on staffing issues last year.

The NHS funding model included penalties for having too many cesareans in a hospital. Funding for maternity was already inadequate and complicated, relying, in many hospitals, on subsidies from other parts of the hospital budget.
Since “Austerity” started, Government funding for the NHS has been inadequate. Staff have kept the NHS afloat through hard work and determination. Staff are worn out. Too many midwives are leaving the profession because of working conditions.
The fight to found the NHS came in large part from the fight for universal maternity care. Let’s make the fight for excellent maternity care in the twenty-first century spur on all our campaigns to protect and improve the NHS
The government does not believe in the NHS. Look at what it is doing to maternity care. Since 2014 they have been working towards privatisation, a US-style model of healthcare. The loss of the NHS or further cuts and privatisation will affect women, babies and maternity. This is the future unless we campaign against it, please join our campaign group – as Nye Bevan said “The NHS will last as long as there’s folk with faith left to fight for it”
We would like to thank https://www.facebook.com/groups/marchwithmidwivesuk for some of these photographs.
See also our earlier blog post,
https://saveliverpoolwomenshospital.com/2022/02/23/weep-for-the-shrewsbury-babies/

Thanks very much for a very useful summary of the most important themes of the Ockenden Report. Staffing levels are so much the key to all the other problems as is the fear of managers and their lack of courage to speak out which leads to bullying and hiding how bad things are. If only managers would work collectively with colleagues to make as much of a fuss as some doctors’ organisations do.
The issue of continuity of carer is very important too – a lot of research was done on this (including by me) and there is poor evidence for the benefits of continuity of care-giver/midwife in labour which is the most difficult part of a maternity service to provide for. it certainly shouldn’t be a priority for maternity care in the current dreadful circumstances and the policy should be halted until/if further research shows that it’s beneficial.
LikeLike
Thank you for your comment. Please do keep in touch. We need to hear from midwives
LikeLike