Protest the damage done to the NHS. The NHS belongs to the people. It should be a public service, not used for private profit. The NHS should be well-staffed and well-funded, with all government NHS funds allocated to patient care, staff, and resources.
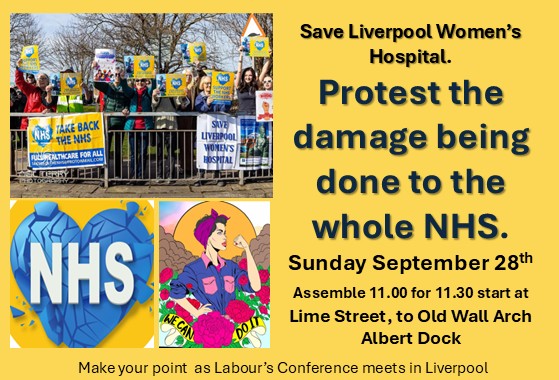
Protest that the NHS should be fully restored and repaired. No more cuts, redundancies or long waiting lists! Improve Maternity services, restore the GP and dental services.No cuts or hospital closures. We protest the damage done to the NHS and demand complete restoration and improvements in the NHS, for all our mothers, daughters, sisters, friends, lovers and every baby.
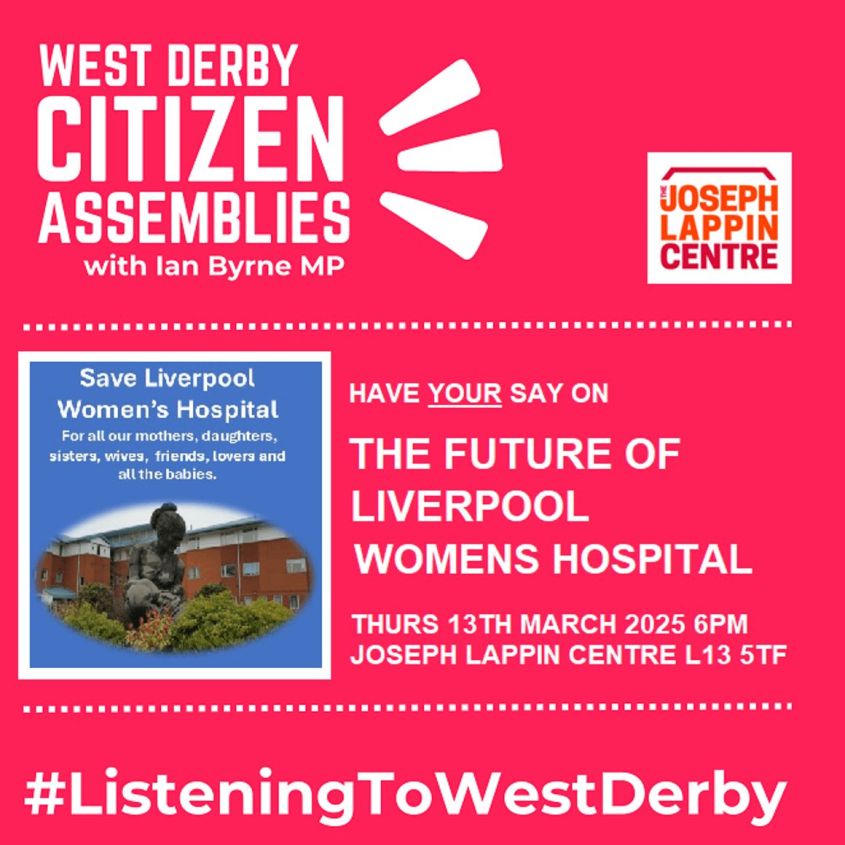
The threats to Liverpool Women’s Hospital are part of the general NHS cuts.

Please join us in this protest on 28th September in Liverpool. As the suffragettes said
“Do not appeal, do not beg, do not grovel. Take courage, join hands, stand besides us, fight with us.”
We are protesting on 28th September when the Labour Party comes to Liverpool for its party conference.
Dr Tony O’Sullivan, Co-Chair of Keep Our NHS Public and retired Consultant Paediatrician, said:
“We’re on the brink of disaster. Everyone knows the NHS urgently needs rebuilding—from staff morale and workforce numbers to crumbling buildings and outdated equipment. Everyone, it seems, except the Labour government.”
It is not just Maternity and Gynaecology care that we fight for; we fight for the whole NHS. Excellent life-saving and life-improving care is delivered day in, day out, by the NHS. Some of it is groundbreaking care, and some of it is more routine. NHS staff work hard with great skill and good humour. Pay the staff well. NHS staff should not need food pantries.

We say “No! to another winter crisis in our hospitals!” Prepare properly, organise the staff resources and the space now! The Government must provide the funds.

The NHS is ours; it belongs to the people.
The NHS is a legacy from the generation that defeated fascism. A legacy from the women who fought for healthcare for mothers and babies throughout the early 20th Century, often while they also fought for women to have the vote, and it’s a legacy all the women who have fought for our rights since then.
The NHS is a legacy of the trade unions that had set up mini-healthcare systems in mining villages, as well as the unions that demanded universal healthcare. The RMT union has helped publish accounts of how railway workers suffered before the NHS was established. The socialist doctors, some from Liverpool, helped shape early Labour Party policy on health. What would they say about the situation we are facing now with a Labour Government doing such damage?
The NHS is a legacy from those who elected the 1945 Labour Government that set up the NHS, while the country was in staggering debt from World War 2. That Government answered to working-class people, improving their lives, not worsening them.
The NHS is a testament to the countless hours of work that doctors, midwives, nurses, and all NHS workers have dedicated to the service, far exceeding their paid hours in both good times and challenging times.
Yes! We can afford the NHS.
This Government’s excuse is the level of national debt. When the NHS was founded, the UK national debt (from war expenses) was 230% of GDP. Today, it is 95%. It is bad for people and bad for the economy to deprive us of good healthcare.
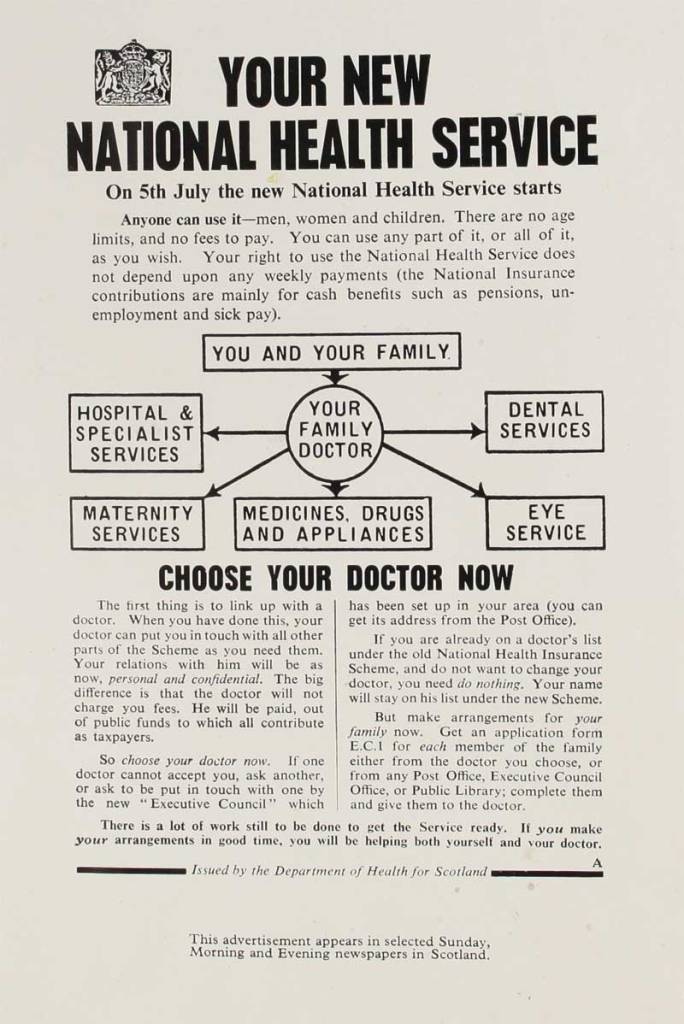
The NHS was founded to be a universal public service, publicly provided and not for profit. The National Health Service provides healthcare to (most) people in the UK, free at the point of need. It is funded by the Government, like other major services.
The NHS faces major cuts and a long process of privatisation, and the use of NHS funding for private profit. Despite facing understaffing, staff redundancies, underfunding, and crumbling buildings, resources are being diverted to profit private companies, including some very unpleasant ones like Palantir.
No one using the NHS faced bankruptcy or denial of services because of medical bills or lack of medical insurance.
There are many ways to reduce the cost of healthcare, starting with better housing, food, access to heating, insulation, and air quality, all of which contribute to keeping people healthy. However, in 2025, we also need investment in healthcare.

We demand an end to poverty. Maternity Action reported from a survey of women on Maternity leave (with a little baby in the house) that:
- One in 10 (10%) of mothers who were using infant formula struggled to afford it. One in four (27%) had cut down on food for the rest of the family in order to buy formula milk.
- Nearly three in five (57%) had reduced the number of hours they heated their home.
- Nearly two in five (39%) had reduced use of electrical appliances.”
Yet most of these mothers had occupational Maternity pay, not just the very minimum the state provides.
UK Maternity services are suffering.
Black Asian and women in the worst off areas re more likely to die in childbirth, or to lose their babies. Liverpool women’s health is set to deteriorate until 2040.
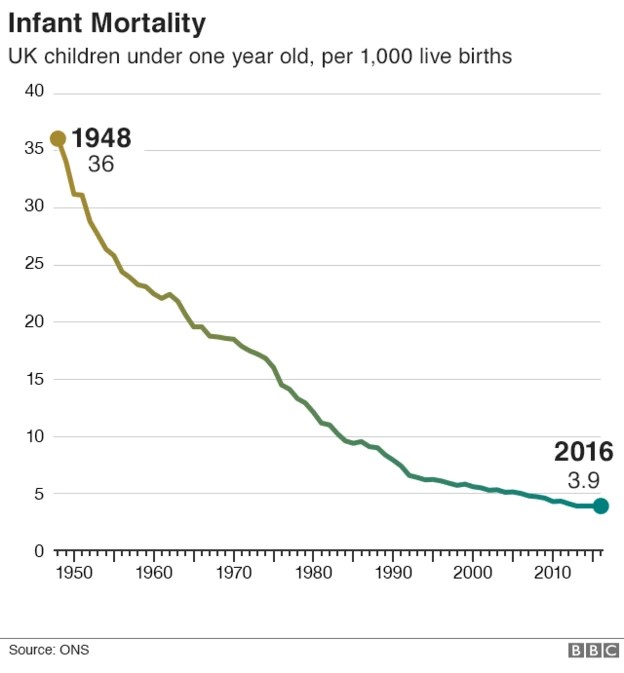
In the 21st Century, the world has made great improvements to Maternity care. In the UK, our maternal and infant mortality rates have worsened while those in other countries have improved.
NHS Maternity is 17th out of 19 comparable countries in infant mortality.
Maternal Mortality is rising, despite fewer births.
The North of England and Black and Asian communities are suffering the worst in infant mortality. In 2022, the UK ranked 19th out of 22 comparable countries, and that has not improved since.
Years of austerity and government cuts have done massive damage to maternity care. Women’s health, life expectancy, and life in good health have all suffered and more so in the UK than in other European countries
What does the NHS do in 2025?
In July 2025, it was reported that each day the NHS provided:
- Over 1.3 million people attend a GP appointment.
- Outpatient Appointments: Over 304,000 people attend an outpatient appointment.
- Emergency Services: Nearly 35,000 people call 999 for an ambulance.
- Major A&E: Nearly 46,000 people attend a major A&E department, with about a third of these patients admitted to hospital.
- Community Healthcare: Over 288,000 people receive community health care services.
- About 1,688 babies are born in England each day,
The NHS is cost-effective and available free at the point of need (to all but migrants, which is cruel and not cost-effective). However, the NHS lags behind other countries’ health systems in the following ways.
- A lack of key resources, including the number of doctors per head of population, the number of hospital beds, and the waiting times for treatment.
- Important health outcomes, such as certain cancers and life expectancy, are worse in the UK.” By 2023, the UK female mortality rate was 14% higher than the median of peer countries, and the UK male mortality rate was 9% higher.”
- Public health issues include housing and food poverty, as well as cutbacks in Public Health Services that work to prevent and control disease. “A report from the UK charity the Health Foundation reveals that public health grant allocations in England have been cut by 24% in real terms per capita between 2015–16 and 2021–22.”
Founded 77 years ago, the NHS fundamentally changed the lives of women, children, and the poor for the better. NHS care outstripped the care previously provided in private hospitals, and the NHS was used by rich and poor, young and old, black, white and brown alike.
Why should we put up with cuts, underfunding, understaffing, and the service being asset-stripped by privatisers?
Every family is affected by the NHS from before conception to the grave. It is with us at our happiest, our most anxious and our saddest times. NHS care affects how long and how well we live.
Grim times for the NHS.
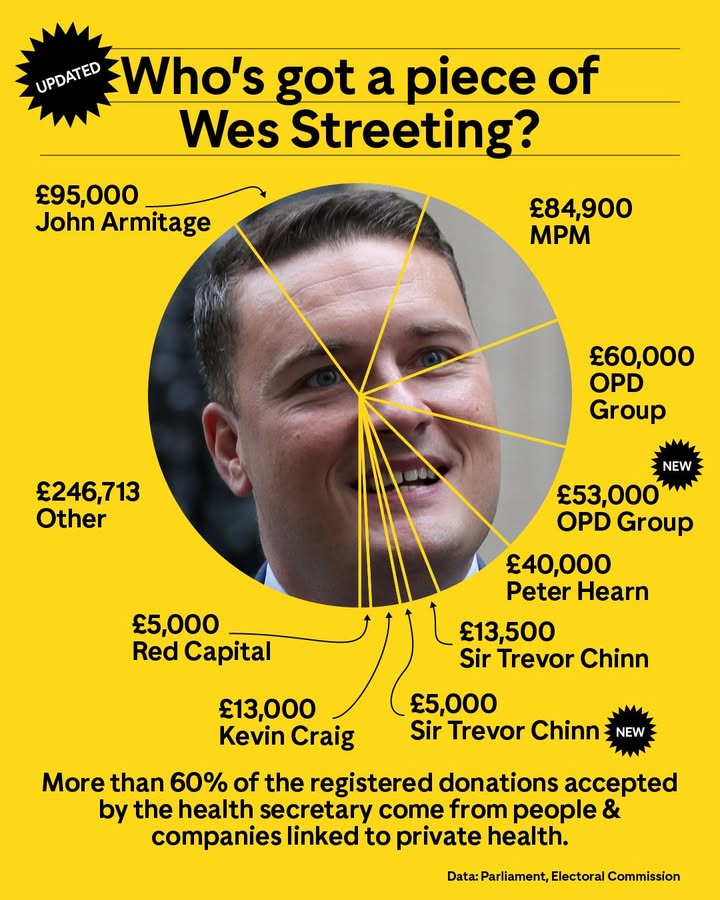
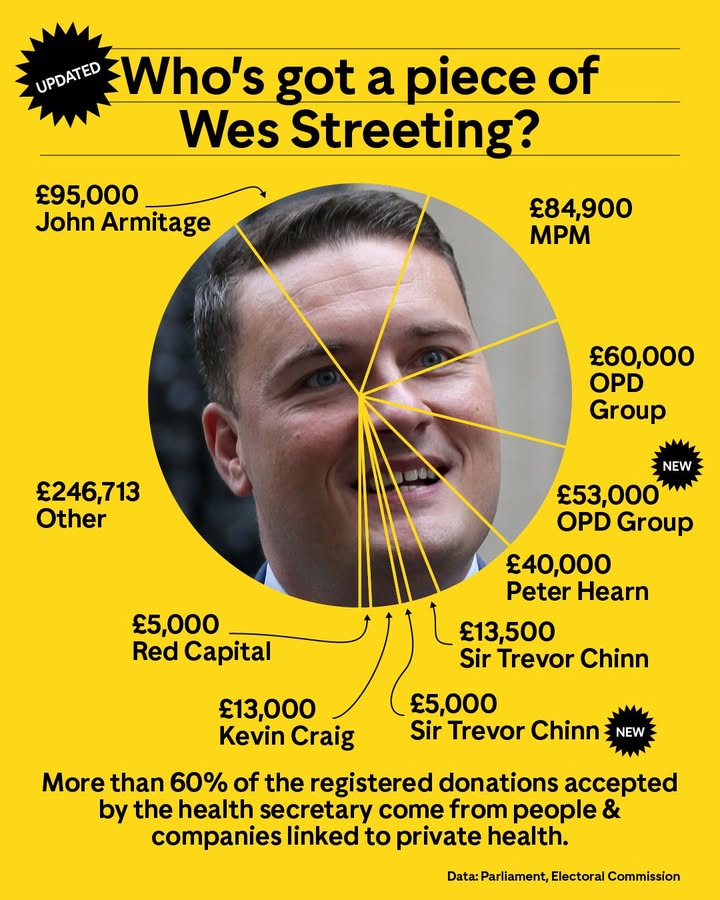
After decades of cuts, privatisation, and money-wasting schemes, such as PFI and Sub Cos, we were promised change for the better, but it has not happened. Could this have to do with the huge donations ministers have received from private health corporations?
We say.
- Restore the NHS as a fully funded universal public service, publicly delivered and government-funded.
- Kick out the privatisers and profiteers.
- Fund patient care to equal the best in Europe.
- Provide the necessary staff. Improve staff pay and conditions. The NHS should be a good place to work, offering good pay, manageable workloads, and time for staff to think.
- Fund the repairs and replacement of the necessary buildings to ensure good, timely care.
- Don’t fund private healthcare or dubious global corporations that are there to make money and make donations to politicians. Pumping money into the private sector damages patient healthcare.
“Our findings show that the private sector is now substituting for, not adding to, NHS capacity.”
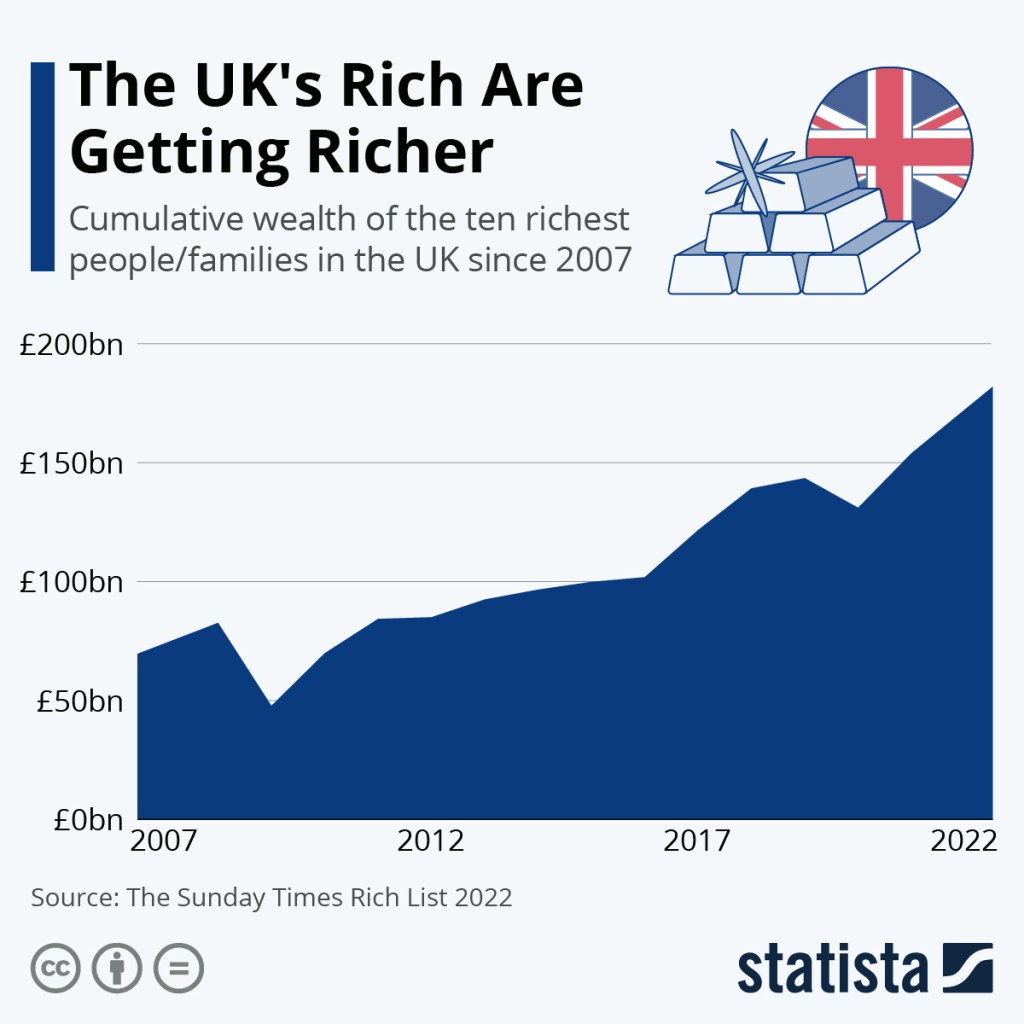
The UK is a very rich country and the rich are getting richer while poverty spreads. It can afford healthcare for all. Indeed, providing universal healthcare is a major investment in the country’s health, wealth and well-being.
The damage done to the NHS over the last few governments is massive. This Government is causing ongoing harm by reintroducing some of the most costly and wasteful (yet profitable for big companies) ideas, such as PFI and Sub Cos.
The (near) universal, free-at-the-point-of-need system in the NHS is an excellent national investment. It gives a good return on the money invested. The cost of collecting fees for health care from migrant workers often exceeds the amount collected.
No solution exists in the US model, regardless of how many government advisers come from that sector. There is a much pushed argument that we can’t afford the NHS, and we should move towards the US health system.US health system corporations are definitely getting claws into our NHS, and they only do that for profit.
In the USA, the Government pays twice as much per person for healthcare. Yet this leaves millions without treatment if they cannot afford the additional insurance. When families can afford health insurance, that insurance can cost as much as their mortgage. Most healthcare plans cover 80% of the cost of care, with the patient paying the rest. What if the 20% is 20% of a very costly treatment like cancer care? One hundred million US citizens owe $220 billion in medical debt. Medical debt can wreck their credit rating and stop them from being able to rent or buy a car on credit.
The USA’s health outcomes are among the worst in the Western world. Maternity and infant mortality are shameful. “The U.S. has the lowest life expectancy at birth, the highest death rates for avoidable or treatable conditions, the highest maternal and infant mortality, and among the highest suicide rates.”
In the UK, we need the Government to;
Reverse privatisation of the NHS in all its many forms
Provide much better funding and staffing in Maternity.
Provide safer, respectful, personalised care for all mothers and babies at every stage of Maternity care.
Bring back quality postnatal care in the hospitals and in the community.
Tackle maternal poverty and food poverty.
End the contract with Palantir, one of the most notorious companies in the USA.
Ban UK politicians from accepting funds from private health corporations or individuals connected to private health or private health insurance.
Fund the NHS to at least good European levels, with all that funding going to the NHS patients, staff, equipment and buildings, not to private companies.
Provide more hospital beds.
“The NHS has a shortage of hospital beds, with occupancy rates consistently exceeding safe levels. The UK has 2.4 beds per 1,000 people; Germany has 7.8 beds per 1000 people. This shortage of beds leads to corridor care”.
Develop a proper workforce planning system, make sure doctors, midwives, nurses and other health professionals have jobs to go to when they qualify. Provide a fully qualified workforce.
Repair our GP service. High-quality healthcare at the GP level should be easily available to all. It is the foundation of good healthcare.
Employ the unemployed GPs. End the power of private companies to buy and run GP practices.
Repair the fabric of our hospitals, clinics and GP surgeries
Bring mental health fully back into the NHS.
Bring dentistry back into the NHS. British Dental Association (BDA) analysis of the data found that nearly 14 million UK adults are unable to access NHS dentistry.
Tackle the waiting lists; don’t fund second-class care in the for-profit sector.
We all need the NHS
From assisted fertility (where needed), to antenatal care, maternity care at birth through postnatal and early years support, through childhood and adolescence, through until old age, the NHS is there to support us. We can all use NHS services, whether in accident and emergency, planned (elective) care, the GP service, mental health services, public health or care in the community. Few are lucky enough still to use NHS dentistry.
If you are younger than 78, you should never have needed to pay for hospital or GP services.
Charges crept in even before austerity for teeth, spectacles, prescriptions and social care. Margaret Thatcher started privatisation in 1982. Her Central Policy Review Staff (CPRS) plan would dismantle the welfare state, scrapping free universal healthcare, forcing people to take out private insurance and charging for education. The CPRS report said, “for the majority the change would represent the abolition of the NHS.” She backtracked when she saw the opposition. She outsourced hospital cleaning, which led to a rise in hospital-acquired infections. Yet even she hesitated to touch the NHS, but later governments have done significant damage.
Social care for our elders was privatised and has become very expensive for individuals and families, unless the NHS pays for it under continuing care. If Social care had been fully nationalised, such payments, either by individuals, families, or the NHS, would not be needed. We would not have been subsidising the profit of hedge funds. Most care homes are private, and many are owned by big business and are very profitable. Much of this profit comes from fees paid by the NHS, local authorities and families. These huge profits are not reflected in the wages paid to staff.
The care provided in our NHS is, many times, excellent, life-preserving, innovative and respectful. NHS staff work hard and often very cheerfully.
Sadly, decades of austerity, privatisation, and mismanagement have caused severe damage to our service.
The 1945 Labour Government founded the NHS. There was hope that it would be improved when Labour won the last election, but we see ongoing damage. Don’t let the damage continue. Save lives—protest for the NHS.
Protest to build a movement like the suffragettes so big the governments are obliged to take action. If enough of us do something about the NHS we can build an unstoppable movement