Restore, Repair and Rebuild NHS maternity care after the Ockendon and Amos reports!
Donna Ockendon who conducted the Nottingham reviewValerei Amos who conducted the national review
In the last week of June, 2026, we saw two hugely significant reports on the damage to NHS maternity services. One report was from Donna Ockendon about long term harm done at Nottingham Hospitals. The other, the Independent National Maternity and Neonatal Investigation, was from Valerie Amos about the situation in ten other major hospitals. The reports describe brutal harm to so many women and babies.
Our love and solidarity go out to all whose pregnancy journey ended in achingly empty arms. Our hearts go out to families who lost their mothers and to the mothers so badly injured physically, emotionally or in their mental health. The additional pain when such an outcome could have been prevented is unspeakable.We send solidarity to those damaged by racism and to those women who were worst off financially and worst served by the Maternity service.
Save Liverpool Women’s Hospital Campaign says;
We demand immediate, significant and lasting improvements in the National Health Service maternity services across the country, in Cheshire and Merseyside and crucially in Liverpool. What we have known from women’s personal experiences has now been presented as formal reports. But many other reports raised the alarm before June 2026. Governments, NHS top bosses and the media knew what was happening long before recent reports and they clearly thought it acceptable, because they let the situation fester.
No ifs, no buts, no whining excuses. Things must change! Invest don’t cut! Babies not Bombs!
Deeds not words are required. We need the spirit of the suffragettes.
The New York Times photo archive via Picryl.com
For all our mothers, sisters, daughters, friends and lovers and for all the babies save Liverpool Women’s Hospital and every maternity hospital and service in the UK!
If these reports are brushed under the carpet as the twenty or more previous reports have been, this harm will be further normalized and the damage extended to ever more women and babies.
There must be immediate,and sustained improvements in the respect given to women, improvements in staffing, in resources, in buildings and equipment, and in management. No more cuts, no more bullying management!
Pregnant women, the communities, and the front-line staff must be included in decisions made about how these these improvements must look and feel.
We stand with the staff who kept the service afloat under terrible conditions. We acknowledge the Midwives who marched in 2022 and who are organising protests this year. We recognise that so many midwives left the profession in protest at the conditions in which women and babies were treated. We demand consequences for the government ministers, the senior managers and senior staff in the higher echelons of the NHS, and in Government, who saw the damage and ignored midwives’ and doctors’ complaints.
To women thinking of having a baby we say that even now most women have good outcomes. Some of the maternity services in the UK provide wonderful service. Do not assume the horrible conditions described in the reports from Donna Ockendon and Valarie Amos represent every birth.If you can, if you have the headspace, we welcome your involvement in this campaign.
We demand safer working conditions and improved staffing for midwives, obstetricians, anesthetists and all the related workforce. The NHS needs more midwives, more obstetricians, and related professions, not as a one off but consistently over a decade.
All those involved in individual acts of cruelty, malice or neglect must be held accountable, but so must the senior administrators and politicians who knowingly allowed this situation to develop and continue.
Britain can afford a good maternity service. Not having good maternity services is far more expensive. Yet in July 2026 maternity hospitals including Liverpool Women’s Hospital are expected to make cuts. How is this justifiable?
The NHS began seventy-eight years ago when the country was far poorer and reeling from the damage – emotionally, physical, and financial, done by World War Two. Our city was one of the worst affected. Liverpool’s children were still playing in bombsites, as the NHS was founded. It is obscene for the government to pretend that today we can’t afford safe care. In 1948 the country decided it was important and invested in the NHS. In turn, this dramatically improved the lives of women and babies.
Women need a greater voice in the service. Women giving birth must be heeded and treated as adults. Women have had to fight for their rights before and will fight now.
The damage to maternity is echoed in so many other aspects of the NHS. We see the overcrowded hospitals and corridor care, the long waiting lists and the over worked staff, the neglected buildings and the money wasted on huge privatisation projects. We see the unfilled vacancies and unsafe cuts. We see the billions handed to big corporations from NHS funds and the unsafe care as treatments are outsourced to for profit companies. Demand that the NHS is restored, repaired and rebuilt!
Join us in campaigning for respect for women’s right to choose their own birth options, more respect for women giving birth, better staffing, and an immediate end to cuts. Every woman and man involved in this campaign helps make the future of maternity better.
Even as Donna Ockendon was conducting her harrowing review into Nottingham’s maternity failings, the local ICB closed the infant bereavement services at the hospital as a cost cutting measure. They knew what Donna Ockendon was doing and still went ahead with brutal cuts.
Don’t think that public indignation alone will make the government take lasting action. Long after the Grenfell fire no one has been punished, nor have other high rise blocks with cladding all been made safe.
Every woman who helps in any little way helps make the NHS safer, makes a difference. We have to build a large movement, deep in all our communities to secure the safety of mothers and babies, and that needs lots of women getting involved.
Fight like your nanas and great nanas did when they fought for and won universal healthcare, free at the point of need.
Mary Bamber, a working class woman fought in Liverpool a century ago for women’s rights and for healthcare for women.
Join us too in fighting for the future of Liverpool Women’s Hospital, the largest maternity hospital in the country. Sign our petition here. At least now the ICB can no longer keep saying integration into a main hospital is always safer. We know of many problems at Liverpool Women’s Hospital, it is far from perfect. However, Liverpool Women’s did not have the bad outcomes described in these reports. We thank the staff for that.
More than ten years ago Save Liverpool Women’s Hospital Campaign was founded to stop Liverpool Women’s Hospital being forced into Liverpool Royal, and to defend maternity services in Liverpool. We have fought on and on. Liverpool Women’s Hospital still on site. The fight goes on to get all the staff and funding it needs but more than 90,000 people have supported us. If you fight you might just win, but if you don’t you will always loose. The struggle for safe and respectful maternity care is a life and death struggle we need to win.
In the 1970s women fought for better maternity care, including letting partners into the Labour Ward, giving women a say in their treatment. That campaign reached many women. We did see change for the better. The charity Aims(Association for Improvements in the Maternity Services) is one of the organisations that was set up in the 1970s during that time of successful campaigning.
Please invite our campaign to come and speak at your organisation, however small. We will publish a more detailed comment on these reports when we as a group have had a chance to discuss them in detail. If you would like to be involved in such discussions please contact us on savelwh@outlook.com or by commenting on the comments section of the blog. For detailed background information see this article from Keep our NHS Public website.
We are campaigning for the best possible healthcare for Women and babies in Liverpool and beyond.The whole of the NHS has been damaged by under funding and privatization. There has been deep disrespect for the people’s health and especially the health of women and babies.The maternity service nationally is scandalously underfunded, understaffed, and under-resourced. Liverpool Women’s Hospital has been under threat all of this time. Our Campaign has fought hard for the NHS and especially for the Women’s Hospital. More than ninety thousand people have signed our petition, both online and on paper. We are still collecting signatures The petition says:
Save the Liverpool Women’s Hospital. No closure. No privatisation. No cuts. No merger. Reorganise the funding structures, not the hospital. Our babies and mothers, our sick women, deserve the very best.
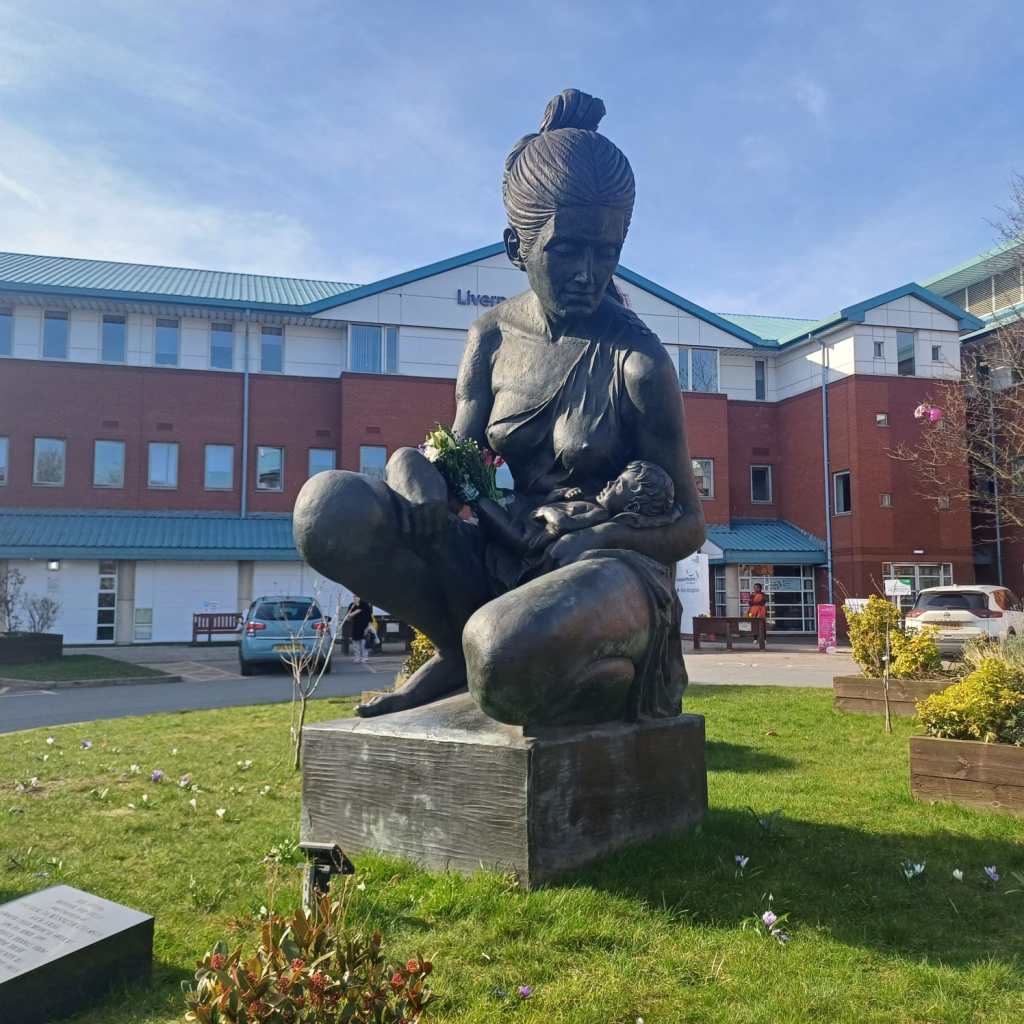
Why is this important? All the maternity and women’s health provision of Liverpool was pulled into this one site. It’s a much-loved hospital. It provides crucial specialised care and the daily joy of new babies.It has a £20 million new neonatal unit and a new diagnostics centre being built. The driving force for closure is a clumsy funding structure, not the needs of women and babies. This is a modern hospital on a good site. and for our mothers, sisters, daughters, wives, lovers, and friends. The alternative wards in the new Royal are not equivalent.
This is a modern hospital on a good site. Our taxes built it for our babies and for our women.
You can see campaigners handing in 20,000 signatures from the petition here.
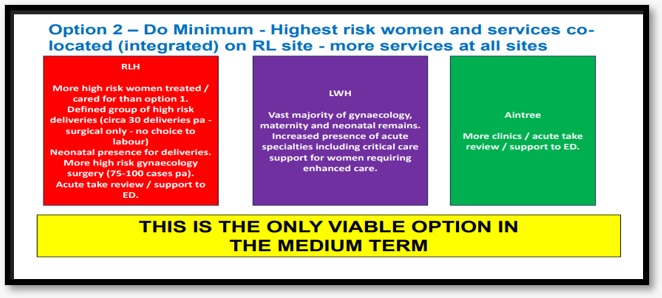
In June and July 2026, the plans for the future of Liverpool Women’s Hospital are out for a public ‘engagement’ exercise. We believe the information being given to the public is inadequate. The process will feature just Option 2. Although a relatively small change, Option 2 is intended to be the forerunner of moving the whole service to the Royal.We say this is unacceptable. These decisions were as plain as the nose on your face at the Cheshire and Merseyside NHS Integrated care Board meeting in January.( The public can attend) These intentions should be made plain to everyone attending the engagement meetings.
This exercise is part of an intention to, over time, move treatment for women from Crown Street. As we understand it from board papers and attending the ICB, the initial group of women to have treatment under this scheme will be the most complex elective surgical cases in obstetrics and gynecology, who need either immediate access to the highest level of long-term intensive care or joint care from doctors with specialism not included in the Women’s.
Emergency patients are not included and cannot be included. They will still need the specialist doctors. We believe short-term intensive care is available at Liverpool Women’s Hospital. Occasionally, a very ill woman might be best served by ambulance transfer to the Royal or another hospital. The Women’s Hospital reported that they are developing a team for deteriorating patients. We hope this is in place quickly because it is much needed. Meanwhile Option 2 does not address the real issues at Liverpool Women’s Hospital.
How to take part in the Engagement about the future of Liverpool Women’s Hospital
Details of how to take part in this very limited public engagement can be found below, but please read our information on the process too. We believe there are significant omissions in the published case.
If you would like to attend the engagement meetings, they are on.
•Monday 15 June, 2.00pm at Merseyside Fire & Rescue Conference Centre, Bridle Road, Bootle, Sefton, L30 4YD
•Monday 29 June, 11.00am at The Old School House, St John’s Road, Huyton, Knowsley, L36 0UX
• Tuesday 30 June, 5.00pm at Blair Bell Room, Liverpool Women’s Hospital, Crown Street, Toxteth, Liverpool, L8 7SS
Information Sessions – Improving hospital gynaecology and maternity services in Liverpool.
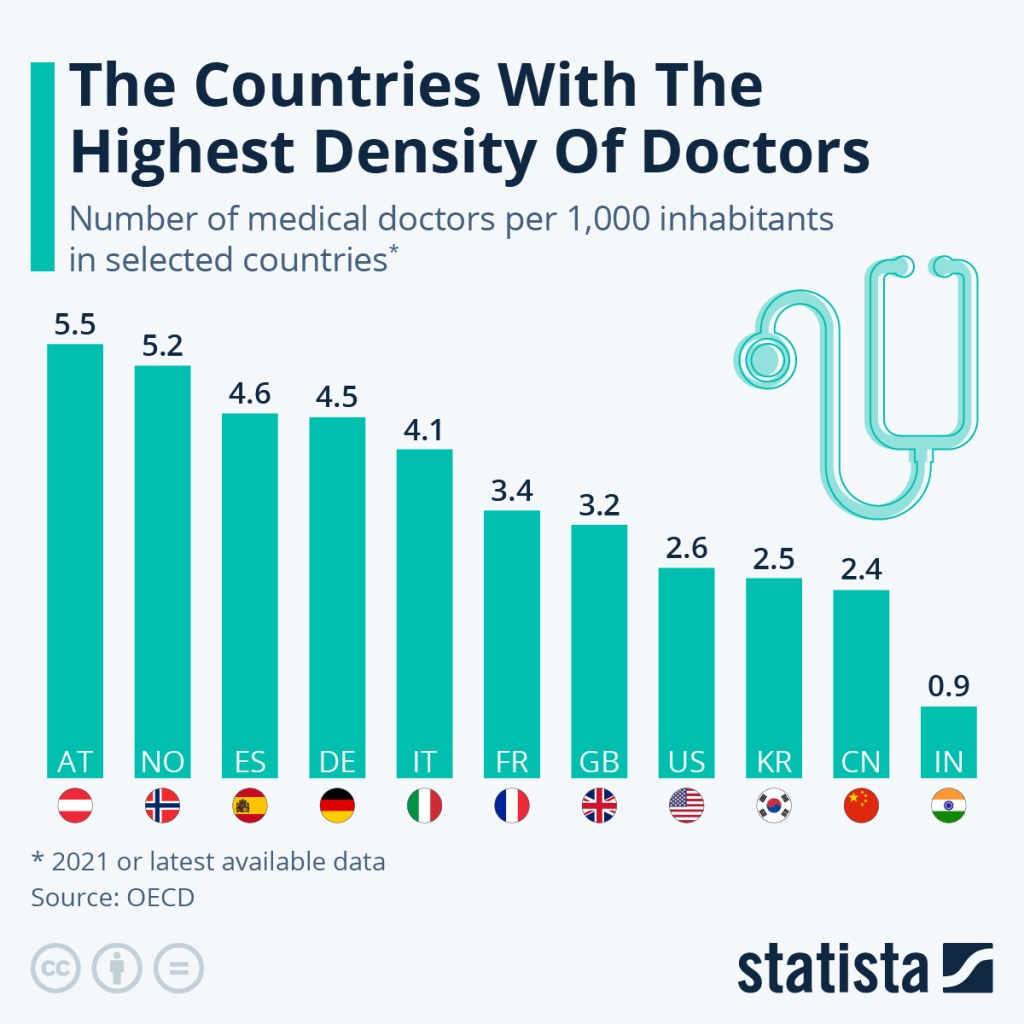
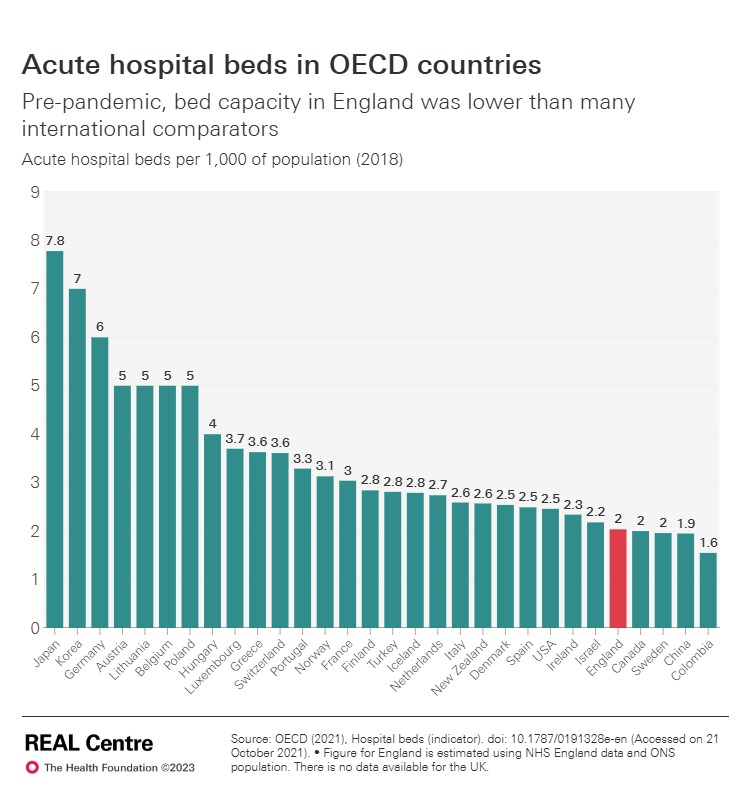
We believe hospitals should work cooperatively, together. The healthcare legislation from Thatcher onward, including the disastrous 2012 Health and Care Act, damaged the natural cooperation between hospitals. Our healthcare has fewer hospital beds per head of population than other advanced countries, fewer doctors per head of population than other countries. To match other countries we would have to hire thousands more doctors. But we have unemployed doctors, The Royal College of General Practice described how qualified G.P.s cannot find posts and the Resident doctors cannot find training posts. This while we need doctors. One in 3 newly qualified midwives cannot find work and other have only part time work. The Independent reported on 4th June 2026 about midwives being told to work double shift with no sleep.
UK needs more doctors!
It does not have to be like this. Such madness must stop. Women say No to this nonsense!
Liverpool Royal Hospital, though new and shiny, and with a great staff, has fewer beds than the hospital it replaced. The Royal is overcrowded, as can clearly be seen in the scandalous long trolley waits in A and E, and in the boarding system, not just during the winter.
Liverpool Royal Hospital photo credit Wikki Commons
Some Women’s Hospital services will be dispersed to other places, including some to Aintree. This will mean reduced services Liverpool Women’s Hospital on Crown Street, and considerable extra management requirements to keep track of all the staff and patients in different places.
This will not improve the issues driving the complaints we hear, nor the ones described at the board, which come from lack of staff and resources, failure to heed women and staff raising concerns, and from disrespect for women or medical misogyny, as the government prefer to call it.
The board of Liverpool Women’s Hospital has given its functions to the NHS University Hospitals of Liverpool Group. That is where board decisions are now taken. There was no public consultation on this. It was driven in part by the acute financial problems at Liverpool Women’s Hospital and at the Royal. That board did not mention maternity in its long term plans at the last board meeting. Maternity should be a high priority in any hospital providing that service.
At a recent NHS University Hospitals of Liverpool Board, the figures for building a new hospital for Liverpool Women’s were given as between £350m and £ 500m, and the cost of making the Crown Street site safer was £6 million a year. So it would take 90 years to be cheaper to build.
We believe the information being given to the public in this engagement is inadequate.
This is not just about some small subset of operations happening at Liverpool Royal Hospital. This is a part of a much larger plan to move Liverpool Women’s services into the Royal.The decisions were made at the January Cheshire and Merseyside NHS Integrated Care Board, the ICB.
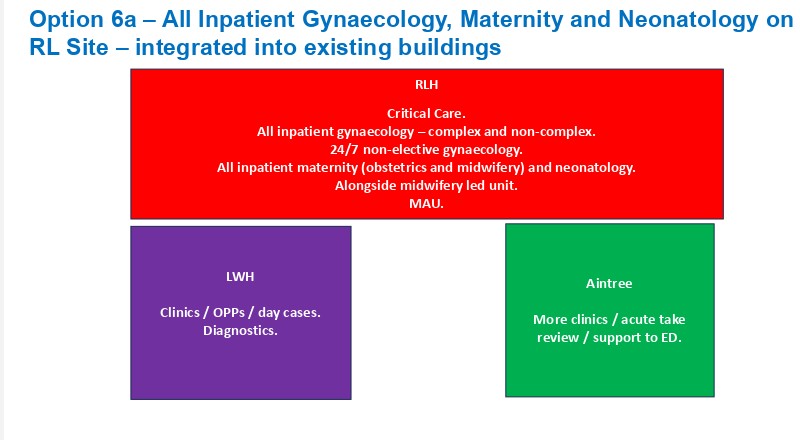
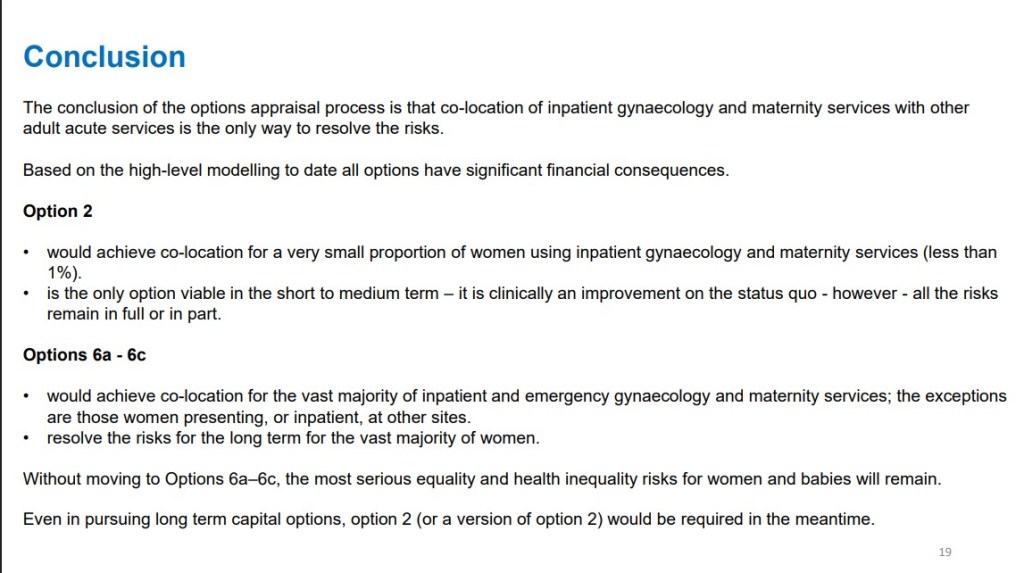
Option 2 is what is being discussed in the engagement process, and bad though that is, Option 6 is the longer-term plan.
The January ICB meeting made it clear (on video 21 minutes -44 minutes in), “…there is no stepping back from the long-term solving of this issue [meaning Option 6] and the need to press the centre and the region for the resource availability and a big capital spend on this…’ ( Sir David Henshaw, the chair of the ICB. This” big capital spend” will compete with other claims on NHS maternity spending.
We published our thoughts here after the January 2026 meeting of the ICB agreed its plans for the future of Liverpool Women’s Hospital, plans we think are fundamentally wrong and impractical. There is no room at the Royal. We need better funding for Liverpool Women’s and better systems of cross-hospital cooperation.
There have been improvements at Liverpool Women’s Hospital,as reported at the last Group board meeting
There are also a set of problems at Liverpool Women’ reported at the last Group Board meeting.
” Risk: LWH does not offer the full range of clinical support services required for delivery of complex and tertiary maternity and gynecology services.Cause: Lack of access to clinical support services at Crown Street”
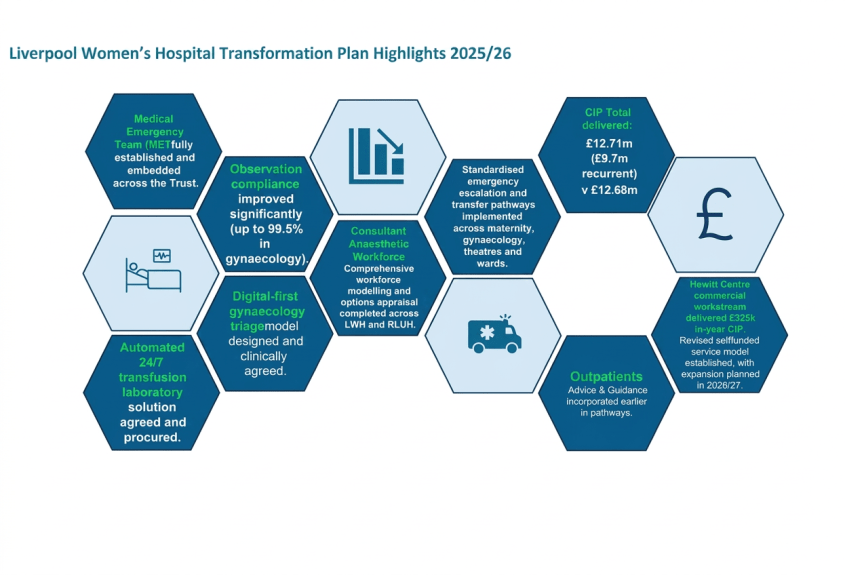
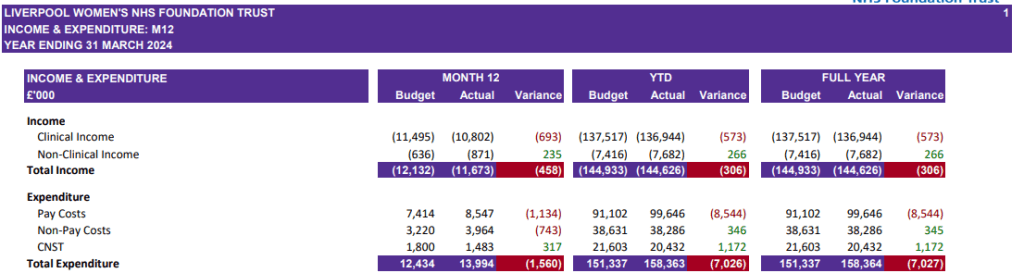
These posts include dietetics, stoma care, occupational therapy, respiratory physiotherapy, dietetics, SALT, pain services and psychology.These are posts that could and should be created. it is not clear exactly why they are not provided at the Women’s but they can and should be so provided. The hospital is in deep financial trouble caused by Government under funding and the particular pressures on Cheshire and Merseyside funding. Other issues have been tackled recently. CIP means Cost Improvement Plans:Cuts to you and me. £12.71 million of them while the hospital lacks some services. The world of NHS cuts is utterly unacceptable
The major maternity crisis in England.
We await two huge reports on the state of maternity care in the UK, one from the redoubtable Donna Ockendon, who has spent two years working on a report from Nottingham. And one from Valerie Amos, who is writing a report for the government. Her interim report was damning. Women want respect in maternity care. The mainstream press is finally picking up what social media and our experiences have been telling us for years. Don’t think for a minute that the politicians and the top NHS bureaucrats didn’t know years ago about the damage going on.
Such is the fear of the state of maternity care that many women are very worried, even avoiding hospital care.
Maternity Buildings are in a poor state.We have a very good building on a good site at Liverpool Women’s Hospital, the Royal is new but not without problems, the Cancer centre is quite new, as is Alder Hey. However the situation in some maternity hospitals is scandalous. Years of Austerity have caused huge damage to the buildings in the NHS.
“Against a backdrop of a £13.8 billion maintenance backlog across the entire NHS estate, over half of organisations reported the formal condition of their maternity and neonatal estate as unsatisfactory, with 42% in need a major repair or replacement and 7% running a serious risk of imminent breakdown.” The Maternity and Neonatal Infrastructure Review Findings report 11th September 2025
Liverpool Women’s Hospital has been affected in the Maternity crisis, with some women, including some of our campaigners, furious over the treatment they received. We are not a fan club for Liverpool Women’s Hospital, nor do we speak for them. We speak for the campaign to Save Liverpool Women’s Hospital. We also have huge admiration for the work of the staff at Liverpool Women’s Hospital, who, despite the difficulties, deliver some excellent service.
Staff have held the service together despite the cuts
We understand they often work with one hand tied behind them due to a lack of resources and management tactics. We are happy to have supported health workers’ picket lines and protests, including the March with Midwives in 2022.
Our Campaign wants Liverpool Women’s Hospital to stay on Crown Street, to be much better funded and much better staffed. We call for it to keep all its services together, on one site (with a better bus service to make the site even more accessible). We want it managed to maximise the health of women and babies. We want all the hospitals to work in cooperation as one health service. But we want to keep the focus on women’s health, and of course, the health of all the dearly loved babies. Splitting the services will cause damage to those services and grief and annoying inconvenience for years to come. Imagine some clinics being at Crown Street, some at Aintree, some at the Royal, and some, God knows where. Imagine navigating that with a baby and a toddler.
Far Worse than inconvenience and thereby missed appointments, there is a very real danger of women’s health issues being further minimised and ignored. That is what has been happening in the NHS (and in other countries that have adopted austerity as policy) for the last twenty years, and these problems have been centred in the big, merged hospitals. The reports of major scandals being investigated by Valarie Amos are in the big hospitals. Leeds and Shrewsbury were removed from the list because of other ongoing enquiries. The 14 NHS trusts are:
Barking, Havering and Redbridge University Hospitals NHS Trust
Blackpool Teaching Hospitals NHS Foundation Trust
Bradford Teaching Hospitals Foundation NHS Trust
East Kent Hospitals Foundation NHS Trust
Gloucestershire Hospitals Foundation NHS Trust
Leeds Teaching Hospitals NHS Trust
Oxford University Hospital NHS Foundation Trust
Sandwell and West Birmingham Hospitals NHS Trust
The Shrewsbury and Telford Hospital NHS Trust
The Queen Elizabeth Hospital, King’s Lynn NHS Foundation Trust
University Hospitals of Leicester NHS Trust
University Hospitals of Morecambe Bay NHS Foundation Trust
University Hospitals Sussex NHS Foundation Trust
Somerset NHS Foundation Trust
The worst-off women, and those from Black, Asian, Gypsy-Romany and Traveller backgrounds, have been most damaged in this Maternity crisis. Please see our earlier posts.
Liverpool Women’s Hospital is at the heart of Liverpool 8 and much loved there. It seems very bad to be damaging Liverpool Women’s Hospital just as these reports are due to be published. A large public meeting chaired by Kim Johnson MP made the opinions of local people very clear.
Liverpool Women’s Hospital is well-loved.
The women of Liverpool have loved the Liverpool Women’s Hospital since it opened, and they loved the previous women’s spaces like Catherine Street and Mill Road. Far too many women experience domestic and sexual violence and are aware, in brain and instinct, of the need for a safe space, organised by and for women, when they are at their most vulnerable. But it’s not just violence – medical misogyny plays a role too.
This love of the Women’s Hospital has a scientific base. The NHS has truly ignored women’s health.
“Women’s bodies have been treated as medical mysteries, not because they are complex, but because they have been excluded. From research funding to clinical trials, a gender data gap runs deep through modern medicine, shaping who gets believed, who gets diagnosed, and who gets left behind.
Less than 2.5% of medical research funding goes to women’s reproductive health – despite women and girls making up more than half the world’s population 1 .
This imbalance is not an accident; it reflects a pattern of medical misogyny, a system that undervalues, underfunds, and misunderstands women’s health.
The consequences are devastating. Women are being dismissed, misdiagnosed, or left in pain for years before receiving answers. Many turn to online communities for help after being told by doctors that their symptoms are “normal”, that they are “making a fuss about nothing”. For people with endometriosis, the average diagnosis time is nearly nine years. Nine years of pain, endless appointments, and disbelief.”
It’s vitally important to keep a women’s space. Not just a physical space, but a place of science and care devoted to women and their babies. A space with a well-qualified and well-treated workforce focusing on women’s health, where women are heeded as women and not dismissed. There is a quiet but fierce rage behind the demands for a woman’s place in healthcare.
No one can deny that the fashion for huge hospitals has at least coincided with real drops in the quality of maternity care and long waiting lists for Gynaecology. These mergers started in the 1990s with the policy of making hospitals work like competing businesses, and then a second wave in 2010 with the Foundation Trust era, as smaller hospitals were pushed into mergers by a financing model that favoured the big hospitals This at least coincided with the deterioration of Women’s health care. Women’s health has indeed deteriorated.
Parliament’s Women’s Equality Committee ( these are MPs, not the government) has twice described the situation for women in great detail but has not been able to secure the necessary funding to improve matters. The first WEC report stated that ‘Medical misogyny’ is leaving women in unnecessary pain and undiagnosed for years”.
We also recognise the importance of the physical environment, and Liverpool Women’s is one of the best hospitals in that respect.
Austerity and political misogyny have a lot to do with the neglect of, and damage to, women’s health. The NHS has been underfunded and consequently understaffed for the years of Austerity, and the future is looking grim too. In 2025-6 and 2026-7, the cuts imposed in Cheshire and Merseyside NHS and through them to the Hospitals and out-of-hospital care are awful. For more details, see this.
Women in England have a life expectancy of about 83 years, but their Healthy Life Expectancy (HLE) is roughly 61.9 years. This means women live upwards of 20 years in ill health.
This is worse in areas where people are struggling with the cost of living, and worse for women with high caring responsibilities, like much of Liverpool, especially where the cost of living is hitting hardest.
And;
“One key point is how females and males differ in many biological and social factors that fluctuate and, sometimes, accumulate over time, resulting in them experiencing health and disease differently at each stage of life and across world regions. The challenge now is to design, implement and evaluate sex- and gender-informed ways of preventing and treating the major causes of morbidity and premature mortality from an early age and across diverse populations.”
The NHS has not done such a good job in the big general hospitals in achieving that understanding, nor in establishing good practice, so there remains a good case for a women’s hospital.
“What happens in pregnancy and early childhood impacts on physical and emotional health all the way through to adulthood the UK dropped from 20th to 26th place (out of 38) in the Organisation for Economic Cooperation and Development (OECD) on female life expectancy between 2000 and 2022. This compares with a drop from 14th to 19th place for male life expectancy during the same period healthy life expectancy among women fell by 2.5 years between 2019 to 2021 and 2022 to 2024”.
Heart and Cancer, too, have neglected women.
It’s not just in the exclusively female aspects of medicine that we see neglect of women. It is true in heart and cancer, too.
There is much written and studied about women and heart disease.
“Recent data published by Professor Chris Galefrom the University of Leeds, funded by the British Heart Foundation, found that more than 8,200 women in England and Wales could have survived their heart attacks had they simply been given the same quality of treatment as men, according to their paper in the journal Heart. The researchers found that women in the UK had more than double the rate of death in the 30 days following their heart attack than men. The researchers suggest that this may be, in part, explained by women being less likely to receive guideline-recommended care.”
Some heart/cardiovascular diseases are exclusive to women and linked to their reproductive health. The improvements must come from all sectors of the NHS.
Women have different heart attack symptoms from men, and it helps if we know these symptoms. It helps if the NHS remembers them too!
Cancer
Several years of National Cancer Patient Experience Survey data shows that women are less likely to be treated with dignity and respect and less able to discuss their worries when receiving hospital care than men – an indictment of NHS culture. The NHS’s inability to listen, itsreluctance to give patients meaningfulpower and choice, and its tendency to disempower patients despite them being the real experts in their own health conditions, is ‘by design’.
They also say, “That is to say, it is a feature of a care model that is:
• one size fits all
• too focused on provider interests, rather than patient interests
• highly paternalistic, centralised and bureaucratic”
The NHS gets a pasting in these reports, but we think something big is missing from the reports.
NHS staff have faced obstacles in getting the resources they need to treat people as they should be treated . Years of cuts, privatisation, and meddling with NHS structure have caused huge damage, and the staff carry no blame for that. Rather, they have worked against the odds to maintain the service.
Lord Darzi, who produced a report about the NHS immediately after the General Election, said, “The Health and Social Care Act of 2012 was a calamity without international precedent. It proved disastrous.” We think the Health and Social Care Act 2022 was another disaster, and Wes Streeting’s sweeping attacks on NHSE and the ICBs have caused another wave of disruption.
We support the original NHS model. This was a universal healthcare service, free at the point of need and paid for by the government. It was a national service with all parts cooperating, but with strong local involvement. Investing in health care makes the economy stronger, not weaker, and helps the population’s health and happiness. Even the right-wing World Bank says so. The wave of privatisation and for-profit companies being involved in the NHS has been an utter failure for patients and staff.
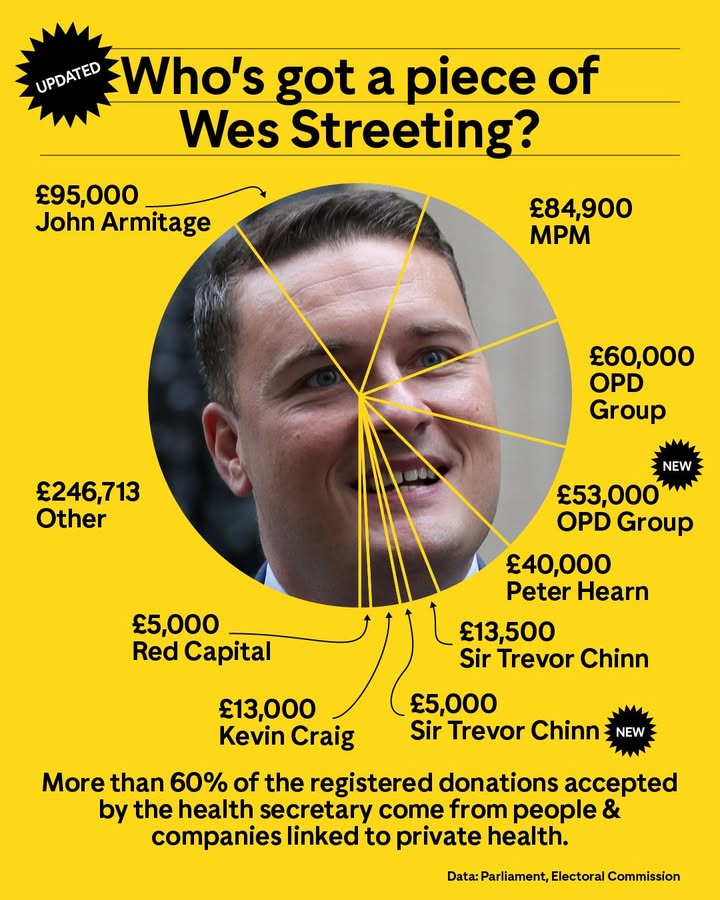
It is a crying shame that Labour politicians, including the not lamented Health Secretary Streeting, have taken money from those who make big profits from healthcare.
The situation in Liverpool is especially serious. In the document Health in Liverpool 2040, it was made clear that the health of women in Liverpool is declining.
“In Liverpool, women can expect to live 57.9 years in good health, and men up to 58.3 years-this means on average women will spend 28% of their lives in poor health, whilst men will spend 23% poorly.
For women, healthy life expectancy is lower than at the turn of the decade, and the gap with England has widened from 5.5 years to 6 years, while for men, the gap continues to be 4.8 years.
“The infant mortality rate has long been regarded as a key indicator of population health that is sensitive to the prevailing socioeconomic circumstances affecting children. In Liverpool, around 26 infants every year do not reach their first birthday.”
“What happens in pregnancy and early childhood impacts on physical and emotional health all the way through to adulthood”
All of this supports a focus on women’s and children’s health, needs currently not being met nationally or locally. This in not to the detriment of men, but because women have different needs
“As we go marching, marching, we battle too for men, for they are women’s children and we mother them again.”
Women also experience sexual and domestic violence, poverty through low wages and inadequate childcare. It takes two incomes to raise a family. Hospitals can only contribute about one-third of what is needed for good health for women. Good affordable food, good housing, clean air, low stress, well-paid jobs, confidence in the future, freedom from assault all help our health outside hospital. But when we as women come into the hospital, it is because we need help. That help must be skilled, respectful, compassionate and well funded.
Too Many Hospitals in Liverpool ?
The NHS seems to believe that there are too many hospitals in Liverpool; they have done for years. The history of this was covered in a Post article called “https://www.livpost.co.uk/a-fucking-feudal-baron-the-long-legacy-of-liverpools-most-feared-nhs-boss/ The article says that a fan of Mrs Thatcher running the local NHS in the 1980s pushed through all the hospitals in Liverpool becoming Foundation Trusts. Liverpool has a different pattern of hospital care from many other cities, and the government wants to change that. It is pushing the ICBs and Hospitals to make drastic cuts.
In 2014, there was a Panorama programme saying that Liverpool has too many hospitals. The next day, it was announced in the Echo that Liverpool Women’s was the hospital that would close.
We started our petition, at first online and then on paper, and we have fought for many years to keep the hospital open.
The process of merging the hospital is underway.
The board-level management of Liverpool Women’s Hospital has been handed, without public consultation, to the University Hospitals of Liverpool Group. However, the Chief Executive of that group has resigned. This coincided with plans to take all Liverpool Hospitals into that group being knocked back nationally. The public now has much less chance to monitor what goes on in Liverpool Women’s Hospital. Board papers cover all the hospitals, There have been major changes in the senior staff. There is no one on the board with a record of work in maternity, nor in Gynecology. The recent long-term plan, discussed in the May meeting of the hospital group, did not even mention maternity or women’s health.
We are now expecting the report on the future of Liverpool Women’s Hospital to appear at the ICB meeting on 29th January 2026. However, other problems may intervene. The winter crisis, staff leaving at the ICB, and the likelihood of major redundancies at the ICB may get in the way. The ICB cannot and should not balance its books. It is in deep financial trouble due to cruel government cuts. The cuts the ICB is expected to make this financial year are brutal. We can see the damage to hospitals across the region. Liverpool Women’s Hospital cannot function long-term without a change in funding that allows for additional staffing and equipment. The two problems, funding for the ICB and funding for the Women’s Hospital, are interlinked.
Investment in healthcare grows the economy. It promotes health wealth and happiness. But that money must get to the staff, patients, buildings, and equipment, not to privatisers providing often substandard care.
Then we have the growing anger from bereaved parents, from women injured in childbirth, from overworked midwives and from the resident doctors. Patients are disgusted by year-long trolley and corridor care in Accident and Emergency, even before the winter crisis. We need more doctors,midwives, nurses and more hospital beds.
Campaigners will be attending the public section of the ICB meeting in January and will report back
What follows is an article from early December 2025.
What’s happening now, in December 2025, with the plans for Liverpool Women’s Hospital?
We stand with NHS workers and thank them for keeping the service going despite the appalling policies from this and recent governments.
Investing in healthcare gives great returns to any country in terms of health and wealth. We ask every reader to help us fight to repair, restore, and rebuild the NHS and Liverpool Women’s Hospital.
Grow our petition! It’s got 84,000+ signatures online and on paper. More will help – it gives the campaign a louder voice with the decision makers. No more Maternity cuts! We need more midwives! Fund Maternity and Gynaecology well across the nation.
For all our mothers, daughters, sisters, friends and lovers and every baby!
We campaign in Cheshire and Merseyside, and many other campaigns are working in different areas. The voices for the NHS and Maternity are growing louder and louder. Please amplify these voices.
Latest news
The ICB (Integrated Care Board ) is the governing body of the NHS in each area. Ours is the Cheshire and Merseyside ICB.
Waiting outside the ICB meeting
At the ICB meeting on November 27th, 2025, which campaigners attended (as members of the public), we were told that the item was not to be discussed, neither publicly nor privately. We had sent written questions. They replied:
“Unfortunately, due to a number of other urgent items which require immediate discussion, the Women’s Hospital Services in Liverpool item will now not be included on the agenda for this month’s private Board meeting, and will instead be rescheduled.“
“When it takes place, the private Board discussion will be focussed on how we move forward with the programme, taking into account the extensive options work that took place over the summer, and will not involve making final decisions about how services might look in the future.”
We had asked in a written question whether the ICB would be discussing the costs for relocation versus staying at Crown Street, as seen in the hospital papers. The additional cost of keeping the dedicated services on Crown Street was described as approximately £6million extra per year. The cost of a rebuild was defined as“up to £336 m- £ 549m“. We pointed out that it would take up to 91 years for rebuilding to be cheaper than providing safe care at Crown Street.
This campaign would like to know what was involved in “the extensive options work that took place over the summer.” We would like to know who was involved in these options and where they were reported, because we cannot find them reported in either the ICB or the hospital board meetings. Why the need for secrecy? Why not involve concerned members of the public? We wrote and asked to be involved in these discussions and were refused. The NHS is not a private corporation; much as some rich companies would like to acquire it, it is still a public body founded by the people, paid for by the people and staffed by the people.
The ICB also said they would still discuss it in private when the item returned to the agenda. We were told there would be some news in the new year. We have also been promised meetings with the ICB chair and the Hospital Group CEO, so we might find out more.
The future of Liverpool Women’s Hospital remains uncertain. What is certain is that Maternity, nationally and locally, must be better funded. It is summed up in a simple fact that we need more midwives.
There is a reluctance in the NHS to say that underfunding and understaffing, too few midwives, and too few hospital beds are core problems. Well, we will say it for them.
Since the 2016 discussion about the future of Liverpool Women’s Hospital, there have been suggestions that it would be rebuilt near the new Royal. Many people still believe this. We neither believe that it will be rebuilt nor support rebuilding it. The Crown Street site is a good building. The staff are a good team with a global reputation. The women and babies of Liverpool need and love that hospital.
Many other Maternity services nationally operate in appalling buildings. The Health Service Journal reported that” Many Maternity and newborn units are at ‘serious risk of imminent breakdown’, regularly hit by leaks and floods, and too cramped to provide the necessary care, an official NHS England report admits. There was a detailed reportpublished by the NHS about this last year. The poor buildings should be rebuilt, not Liverpool Women’s Hospital. Many other hospitals urgently need a rebuild, but the plans for that are delayed.
Improvements at Liverpool Women’s Hospital
There were reports last year that a deteriorating patient’s team was being developed at Liverpool Women’s Hospital, and we hope that this is now in place. This is much needed. Other improvements are in place, including bringing the “soft facilities management services” (cleaners, porters, etc.) back in-house. The Case for Change states that “As part of elective recovery funding, £5m has been provided to establish the Liverpool Women’s Hospital site as a centre for gynaecology procedures. This includes four state-of-the-art procedure rooms developed to free up capacity in theatres and create additional clinic space for more minor operations, and will enable up to 4,200 additional gynaecology procedures every year.In addition, Crown Street now hosts a community diagnostics centre with CT (computed tomography) and MRI (magnetic resonance imaging) from 8am to 8pm, and urgent access to CT 24/7, which has delivered improved access to scans and reduced transfers for these diagnostic tests.
From an exhibition at the celebration of 30years at Crown Street, (Our Photograph)
The CQC report in August 2025 stated that Liverpool Women’s Hospital has improved.
“Karen Knapton, CQC deputy director of operations in the north west, said: “We were pleased to see that leaders and staff working in Maternity services at Liverpool Women’s Hospital had acted on our feedback from the previous inspection and worked hard to make improvements. Women and people using this service now had a much safer and improved experience of their care and treatment. Behind this was an improvement in how well-led the service was, which in turn supported staff to provide better care.
“For example, it was positive to hear that leaders had improved staffing levels. Women using the service told us there were enough staff to meet their needs, and they were treated with compassion and kindness. It was great to see this reflected in a recent people experience survey, which found 94% of women felt they were treated with respect and dignity.
“Overall, the Maternity team at Liverpool Women’s Hospital should be proud of the improvements our inspection found. They should use them as a foundation to keep building on.”
We applaud these improvements. Nowhere does the CQC mention relocation, nor have earlier, less complimentary CQC reports mentioned this.
Underfunding and understaffing have caused severe damage to mothers, babies and staff. More has been paid in damages from the service than has been spent on the whole national Maternity service.
Scandalously, “the potential cost of Maternity negligence claims in England since 2019 has reached £27.4 billion, which significantly exceeds the estimated £18 billion budget allocated to Maternity care over the same period“. We say improve the services and reduce the damage! When will the government focus on the needs of mothers and babies?? The voices of women and their families must be even louder on these issues.
Co-location has not been a success for maternity. It is not the only problem, far from it. Cuts and underfunding have been a disaster.
The “Case for Change” also says, “All other specialist centres for gynaecology and Maternity services in England have co-located acute and emergency hospital services.” We say that this co-location of Maternity in general hospitals has not proved to be a cure-all for Maternity crises, far from it. Maternity, despite being based in acute and general hospitals, is in crisis.
Although a standalone site, Liverpool is not one of the 14 Maternity providers involved in the so-called “rapid” national investigation of Maternity and newborn baby care across England. The Labour Government promised a rapid enquiry, but this enquiry is now not reporting before Christmas and might report sometime in the new year, and will not hear from bereaved parents.
Fourteen general hospitals ARE included in the national Maternity crisis, and others have been the site of some of the Maternity scandals. The Shropshire Okendon enquiry indicated that the management did not give Maternity due attention, nor did the Morecombe Bay hospital management give Maternity due attention, even after the big report.
It’s not just Maternity that is suffering in the NHS.
The women’s hospital reflects the many problems besetting our healthcare system. Books have been, and will be, written about this. We are trying to change the situation. These are the core issues.
For many years now, the NHS has been underfunded and understaffed compared to other countries, and this has been a clear government policy.
The organisation of the NHS has been damaged by pro-market legislation, especially the 2012 and 2022 Acts, which set hospitals up to compete against each other and allow for-profit interests to have a much greater say. Lord Darzi, in his report for the incoming Labour Government, described the 2012 Act as a“calamity without international precedent” that “proved disastrous”. For Liverpool Women’s Hospital, it meant that cooperation between hospitals proved very difficult, and the high cost of the foundation trust system was too much to bear. Not keeping to an impossible budget made them constantly under pressure.
Maternity and gynaecology, across the country, suffered badly, with one in six Maternity units closing, and standards deteriorating. A major Maternity crisis developed with standards and staffing suffering, resulting in damage to mothers and babies.
What were the greater issues that pushed the Liverpool Women’s Hospital to the back of the agenda? They were hugely based on funding, cuts and the winter crisis. We will write about them in another article soon.
“You get one chance to deliver a baby safely. There are no reruns or repeats. The accoucher must get it right every time. To do so, the midwife must be supported by her colleagues, midwifery management and work within a fully safe environment. Alas, with the fragmentation of our NHS, top-down draconian management, our mothers, their babies and our midwives are given short shift, and they become the victims of often tragic circumstances.There is a woeful shortage of skilled midwives. Anyone can deliver a baby, but it takes a skilled midwife to do so day in day out safely and with professional accountability,” from our campaigner Stephanie (below)
Campaigner Stephanie, one of the generation of midwives who say they worked in the golden age of the NHS. We fight for another golden age. Join us
Use the links if you wish, but they are not essential to understanding the information.
The campaign wagon that we use when we can collect enough donations.
NHS University Hospitals of Liverpool Group Board meeting.
As members of the public, we have attended the ICB and the Liverpool Women’s Hospital Board meetings for some years and attended the NHS University Hospitals of Liverpool Group Board meeting on June 5th, 2025.
We heard that because the ICB was refused the funding it requested, all Cheshire and Merseyside Hospitals and many other services must change their financial plans for the worse. However, the Trusts are not allowed to reduce their planned services! This must increase pressure on the frontline NHS workforce. Staffing is a large part of all NHS spending and is crucial to patient care.
Note: “Cost Improvement Plans” are cuts. Yes, a large organisation like the NHS must be on the watch for potential savings, but the system is used to enforce cuts.
The ICB reported that “On April 30th 2025 the ICB submitted a compliant plan ( which has resulted in both the ICB and every Cheshire and Merseyside Trust provider taking on additional cost improvement requirements (resulting in an aggregate deficit across the 16 NHS providers of c£228m offset by a surplus for the ICB of £50m). This compliant plan will enable us to spend our allocation, plus the additional £178m of deficit support funding (equivalent of 2.2% of our allocation) during the2025/26 financial period. Whilst agreeing a plan was essential to securing the deficit support and cash to underpin this, our attention must turn now to the effective delivery of the plan and effectively mitigating the risks“.
Like Oliver in the workhouse, the ICB asked for morePicture credit
See our commentary on the May 2025 ICB board here.
We have always opposed the ICB system imposed by the 2022 Health and Social Care Act. Streeting is giving us more of the same.
We have observed how trusts negotiate their funding with the ICB. They agree on a plan for services, treatments, and the required money. It is a complex operation with oversight from outside bodies. The ICB takes all the plans for all the services in the area to NHS England and agrees on funding levels. Negotiations continue during the year for next year’s funding. The NHSE rewards trusts that do well in certain areas and has just announced some capital funding for buildings and extra services, including mental health in the acute hospitals. This, though, we are told, is not additional money. This carrot-and-stick funding is inappropriate and wasteful; it just lets a few positive headlines help some MPs.
The ICBs ( separate and distinct from the Hospitals and provider services) facesignificant cuts in their functions and funding as Wes Streeting implements his peculiar plans for the NHS.
The Health Service Journal reports that his year, “Integrated care boards and trusts are collectively aiming to make efficiency savings of 7.1 per cent or £11bn.”
These cuts are imposed while the winter crisis in our hospitals lives on through the summer in some places and is unlikely to improve next winter. At the same time, we have unemployed GPs, people needing GP care, and more than six million people waiting for treatment.
Women’s health sees some of the longest waiting lists, and our Maternity outcomes urgently need to be improved. Women hold up half the sky and make up nearly 80% of the NHS workforce. They are more likely to think of the NHS when voting. Yet our healthcare is disrespected in so many ways. The country has a Maternity crisis, and mental health care is severely damaged.Social care is a disgrace.
Liverpool Women’s Hospital is now part of the NHS University Hospitals of Liverpool Group, which comprises The Royal, Aintree, Broadgreen, and Liverpool Women’s Hospital. Other Liverpool Hospitals will also join the Group soon. “Liverpool Heart and Chest will join by September this year, the Walton Centre by December, and the Clatterbridge Cancer Centre by March 2026.”
(No, you didn’t miss the public consultation about the creation of this Group because there was none.)
Liverpool Women’s Hospital is still technically a separate Trust; however, the final say now rests with this group board, none of whom, as far as we can tell, have obstetric or midwifery expertise.
“Although LUHFT and LWH will remain in operation as statutory entities, in all other aspects, they will delegate authority to NHS University Hospitals of Liverpool Group (UHLG)”.
Hospitals receive funding via the ICB. They also agree on their planned treatments and urgent and emergency care Plans with the ICB. The Trusts are paid for what they plan to deliver.
The Trusts and the ICB had drawn up these plans in detail. NHSE had appointed outside bodies, like Price Waterhouse Coopers, to work with the Liverpool boards and the ICB to oversee their finances and to reduce spending. It was just such a worked-out package that NHSE declined. Further, NHSE would withdraw previous deficit funding of over £176m to Cheshire and Merseyside if the books were not balanced. Each Trust was given far less money than they expected.
The CEO of the Liverpool Group explained that, having received less funding, they had to decide which services to cut. But, they were then told they still had to meet the original service targets with less money.
So, Liverpool Women’s Hospital is facing more financial problems. It is a small hospital whose funding is determined by the Maternity tariff, and the Maternity tariff( funding) is inadequate across the country.
These national cuts are a policy decision distinct from previous years. They come after years of Austerity, privatisation, and underfunding in the NHS. Sadly, this Government’s policies are little different from the last.
Campaigns do make a difference. If you fight, you might just win.The more people involved, the more likely we are to win. So, we have to campaign harder and draw more people into the campaigns to Restore and Repair the NHS.
The NHS came from ordinary people, unions, women’s organisations and community groups. That is to whom we must turn again. Please join the campaigns to restore and repair the NHS. Contact us for details on how you can help.
There may well be some waste and overspending in the NHS. These cuts happen while more than six million people are waiting for treatment. Some treatments, like those for endometriosis and young people’s mental health, need to improve. We need democracy and community oversight in the NHS.
When our campaigners go to meetings and read their papers, we still have limited sight of what’s going on and only retired people really have the time to attend these meetings.
On June 5th, we could not even hear crucial sections of the meeting where significant changes in the funding and delivery of services were being discussed. We were “told off “for asking them to speak up in what is supposed to be “a meeting held in public.” They have promised to use microphones at the next meeting. There is no effective democratic scrutiny of the NHS.
This new board format shows less detail of Liverpool Women’s Hospital matters. We do not, for example, see the staffing fill rates for different services as an issue that matters very much to women giving birth. From the reports that we did see, we learned that Liverpool Women’s Hospital has a significant waiting list for Gynaecology treatment:
“Gynaecology remains a challenged speciality nationally in terms of long waits and capacityconstraints. At LWH, referrals into the Gynaecology suspected cancer pathway havesignificantly increased over the last 3 years, increasing from 3,500 per year in 2021/22 to 6,000 per year in 2024/25 – a 71% increase. Demand has been exacerbated by changes in the Post Menopausal Bleeding pathway as well as significant long waits for General Gynaecology services. LWH is also the Tertiary provider for Gynaecological Cancer across Cheshire & Merseyside.” Page 239 in the Board papers
The hospital is opening three new “ambulatory” (daytime) treatment rooms. However, increased demand has already shown a need for still more capacity and money to fund that capacity. We were told that close work with other cancer teams across the Group and support from across Cheshire and Merseyside are helping to develop an effective plan to drive down this waiting list.
Gynaecology has one of the longest waiting lists across the country.
In March 2025, Endometriosis UK wrote New data shows the non-cancer gynaecology lists continuing to stand at over 580,000 women in England alone, with women waiting months and even years with serious, progressive conditions, including endometriosis.
In December 2024, The Guardian wrotethat waiting lists for gynaecology appointments across the UK had more than doubled since February 2020. Records show around three-quarters of a million (755,046) women’s health appointments are waiting to happen – up from 360,400 just before the pandemic..
The NHS should be a nationwide, publicly delivered, well-funded and well-staffed service. Our campaign always called for cooperation between hospitals and rejected the Conservative ideas of competition between hospitals and bringing the market economy into the NHS.
Unsurprisingly, pressure is being put on the workforce to work harder. All kinds of stunts are coming in, like outsourcing, insourcing (not the same as bringing services back in-house), changing how bank nurses are paid, not filling vacancies and more privatisation. Privatisation is not more cost-effective, nor does it deliver better patient outcomes. Services, too, will be cut.
It is unacceptable that the Government is imposing such a scale of cuts while we wait for treatment.
We learned little of the plans currently being drawn up for the future of “Women’s Hospital Services in Liverpool”. We questioned whether staff at LWH had been told that one option was a new build on the Royal site. It seems it was mentioned at a staff briefing, but only as a reference to the options years ago. The ICB had categorically ruled out a new build for Liverpool Women’s Hospital on the old Royal site, and the site has been agreed upon as a new building for the university. The Echo reported on June 5th about more details for the site of the old Royal, including an improved entrance to the Royal Hospital. There is no mention of a rebuild for Liverpool Women’s Hospital, although plans can change until construction starts.
We want the Liverpool Women’s Hospital to be properly funded and staffed and to remain on the Crown Street site in cooperation with other hospitals.
“Save the Liverpool Women’s Hospital. No closure. No privatisation. No cuts. No merger. Reorganise the funding structures, not the hospital. Our babies and mothers, our sick women deserve the very best.”
Why is this important?
All the maternity and women’s health provision of Liverpool was pulled into this one site. It’s a much loved hospital. It provides crucial specialised care and the daily joy of new babies. #one born. The driving force for closure is a clumsy funding structure not the needs of women and babies. The alternative of wards in the new Royal is not an equivalent.
This is a modern hospital on a good site. Our taxes built it for our babies and for our women.“
We campaign to save Liverpool Women’s Hospital, to Restore, Repair the NHS, and to make the NHS a great place to work. Please help. Combining our paper and online petitions, we have 81,470 signatures. Please help us get even more. Our work includes petitions, leaflets, stalls, rallies, working with other Maternity campaigns and with community groups, unions, Keep Our NHS Public, and other NHS campaign groups, our Facebook page, and this blog aims to provide information and help campaign organisation.
Proposals for the future of Liverpool Women’s Hospital seem likely to be published before the end of the year. They will then have to go to a public consultation.
We heard on our stalls that staff at Liverpool Women’s Hospital had been told that the hospital would be rebuilt on the site of the demolished old Royal. We asked the ICB, “There is mention of a meeting with the LWH staff to reassure them about the process. Was there mention of the likelihood of funding for a new building on the Royal Site? We have been told that this happened, but this contradicts earlier statements from this board. ”
We asked the Hospitals Group board,” Regarding Women’s services in Liverpool, has the suggestion of a new Liverpool Women’s Hospital at the Royal site been raised with staff either at the Royal or LWH?“
The ICB answered. “There was a staff engagement event in February 2025. This event was to update staff on the progress and next steps of the programme i.e. the development of an options appraisal process. Consideration of the funding requirements are a part of that process for developing potential options to address the risks identified; this will be both capital and revenue costs. This was discussed in general and hypothetical terms only,as no funding decisions have been made at this point.”
We need clarity on this. If staff are being reassured by ideas of a significant new build, an idea that contradicts what the public has been told repeatedly, there is a lack of clarity.
Meanwhile, the fight to protect and improve healthcare for all our mothers, sisters, daughters, friends, lovers, and every baby continues in these grim circumstances.
Our grandparents and great-grandparents fought for and won the NHS as healthcare for all, free at the point of care, publicly provided, funded by the government, providing the best available treatment in a timely fashion. The impact of the NHS on women’s lives was profound. The NHS was won at a time of hardship in the British economy, when Liverpool and other cities were still full of bomb sites. Our current period of cuts and closures, of declining outcomes and greater birth trauma, is robbing us of the legacy left to us by the generation that defeated fascism. Fight for our healthcare like your grandparents, great-grandparents, and even great-great-grandparents. In the early 20th Century, the working-class women of Liverpool fought long and hard for better healthcare and won it. We can do that too.
We fight for Liverpool Women’s Hospital and to Restore and Repair the NHS.
Day by day, the NHS provides services for patients often with great skill and good humour. Despite years of cuts, the NHS survives but it cannot provide all services we need because of austerity and the privatisation agenda.
We are in grim times, but the fightback is growing. Our petition has reached 76,000 signatures. We have had support to pay for our leaflets and meetings. People who spoke at the engagement meetings unanimously supported keeping Liverpool Women’s Hospital. Not a single member of the public spoke in favour of closing it, or dispersing its services. We have great support from the public, and two Liverpool MPs, Kim Johnson and Ian Byrne, have helped this week. The same day as the ICB meeting and the first joint board meeting of LUHFT and Liverpool Women’s Hospital, Kim Johnson raised the issue in Parliament. Ian Byrne sent a great letter to the Engagement Team, saying “NO!”.
However, the process decided by NHS bureaucrats rolls on. We can stop it if we organise.
The many people who have said “that will never happen” should join the fight back.
Two quotes show the seriousness of the threat we face
At the October 9th meeting of the ICB Fiona Lemens, leading the process said, introducing the engagement, “It’s too early in the process to speculate about how services might look, in the future at the Crown St. site and across the city, because we’ve not started that design work yet, but what we can say is that we need that hospital at Crown St. The things that we could consider that we currently need space for would be out patients, day case procedures. We’ve invested in a CDC, we need that diagnostic capacity for the patients in Liverpool, and this is an excellent building to provide that from and we are absolutely committed to NHS delivered services being delivered from that site, and there are no plans to discuss any other forms of services going in there.”
So, Fiona, where will our babies be born? Where will the women of Liverpool receive their gynaecology care? Where will fertility go? Where will genetics go?Where will the Bradford clinic go?
The website for Liverpool Women’s Hospital says about the second strand in this threat to the integrity of the Women’s Hospital, the largest maternity facility in the country :
“From 1 November 2024, Liverpool Women’s NHS Foundation Trust became part of NHS University Hospitals of Liverpool Group (UHLG). UHLG has been created through the coming together of Liverpool University Hospitals NHS Foundation Trust (LUHFT) and Liverpool Women’s NHS Foundation Trust (LWH).
Please note, Liverpool Women’s Hospital is now represented on the Group Board of Directors of NHS University Hospitals of Liverpool Group (UHLG). Details of past Liverpool Women’s NHS Foundation Trust public board meetings can still be accessed via the links below.“
On Thursday 28th November 2024, two crucial meetings happened. These meetings were:
1) The ICB meeting which received the first report of the Engagement process to decide the future of the Liverpool Women’s Hospital, discussed the winter crisis, and how to handle their lack of adequate funds. We, as members of the public, asked questions. We were told that the first response to the engagement would be reported in February or March. They are paying £24,000 to a company called Hood and Woolf to produce the report on the engagement.
We also learned of the grim financial position, and the situation regarding the terrible winter crisis, likely to be worse than last year. There will be a full report on this in a later post.
2) The inaugural meeting of a new joint committee, which has the delegated powers of the boards of Liverpool Women’s Hospital and the Liverpool University Hospital Foundation Trust (which covers the Royal, Aintree and Broadgreen). We fear that maternity will be treated as badly as maternity has been treated in so many other big acute hospitals, leading to major problems and major enquiries.
This joint committee of LUHT and LWH, also reported that the winter crisis is starting (staff tell us it started a while ago). They also discussed services that might be moved to, or from, the Crown Street site although such moves were already a fait acomplis, and the integrity of a Women’s Hospital seemed to be already lost.
We think it’s wrong that while the ICB follows a protocol to consult on service changes, the merging of the hospitals had no consultation whatsoever, and precious little discussion at the Liverpool Women’s Hospital Board. We were told at the engagement meetings, that merging hospitals does not need public consultation. This huge change was just ‘steamrollered’ through. Merging the Women’s is just the start. The intention is that the specialist hospitals in Liverpool, the Clatterbridge Centre, the Walton Centre and Broadgreen Heart and Chest, will be pulled into an even bigger merger. In contrast to LUHFT, the specialist hospitals have been funded nationally and do not share the financial crises facing LUHFT. It seems odd to us that such major reconfigurations are not considered to require public consultation, while (albeit cruel) changes to such things as celiac prescriptions do. At the ICB it was announced that they are going out to public consultation on whether prescriptions should still be available for gluten-free products for celiacs (A Gluten-free loaf can cost as much as £3.99.) We think this cut is terribly wrong for people already hard up, and struggling for enough food. Many celiacs don’t ask for prescriptions but the damage of this policy will hit the poorest hardest. The Celiac prescriptions cut is yet another cut amongst many – but surely, if this merits consultation, so must merging hospitals?).
Our campaign wants a well-staffed, well-funded Women’s Hospital on the Crown Street site. We want maternity to be funded and staffed well across the UK. We say enough of maternity scandals, enough of birth trauma, and enough of closures and cuts. We say this for all our mothers, daughters, sisters, friends, lovers, and babies. So many other countries do so much better than the UK in maternity and infant mortality. Once we were up with the best but austerity has damaged the service costing many of our babies’ and mothers’ lives, and women’s health.
We have 76,000 signatures on our petition to save Liverpool Women’s Hospital. People sent in many postcards opposing the idea of closure, or dispersal of services as set out in the engagement.
You can read more about the “engagement” process here from Greg Dropkin of Keep Our NHS Public.
We want to restore and repair the whole NHS, and to stop the relentless”Winter Crises”.
The NHS was founded to provide:
A national public service providing healthcare for all, free at the point of need, government-funded, publicly run, and publicly delivered, with well-qualified staff. For decades it worked very well, being declared the best health service in the world. Now it is seriously damaged and must be repaired.
The NHS came from decades of campaigning by working-class women, like the Cooperative Women’s Guild, and the Trade Unions, not from the rich and powerful. If we want to keep it we too fight for it.
The NHS has seen reorganisation after reorganisation in favour of the American model, most recently the Integrated Care Model. The ICB for our area is called Merseyside and Cheshire ICB. This body controls the allocation of money to the hospitals and policy over cuts. Cheshire and Merseyside ICB, and other ICBs simply do not have enough money to function properly. They were conceived as part of a hospital closure project, to reduce the costs of the service and make it more acceptable to US health corporations take-overs. There are other hospital closure plans still going on, as well as the threat to Liverpool Women’s Hospital.
The ICB conducted an “engagement” with the public about the future of Liverpool Women’s Hospital. It was not well publicised but did include four in-person meetings for which they asked people to register. In all four meetings, their proposals were roundly rejected, but the attendance was small, very little effort was put into getting real engagement. We will write more about this in another post. None of the meetings were at a time suitable for working mothers to attend.
What you can do to help
Help with the campaign distribute leaflets and help getting the petition signed.
Raise it with your trade union, or other organisation
Tell your MP and councillor Liverpool Women’s Hospital must stay at Crown Street as a full women’s service run by experts in women’s health, in maternity and related services. Tell your MP that hospitals must cooperate not compete or merge.
Tell them that the winter crisis is unacceptable. Tell them that problems including finance, staffing, buildings and equipment must be sorted and the drain into private companies must stop.
What has Liverpool’s “Place” NHS and Cheshire and Merseyside ICB done whilst maternity care nationally is in a well-publicised crisis and thousands of women are furious about the level of care they and their babies received? While the public enquiry into baby deaths at Countess of Chester has just opened? While Alderhey is at the centre of the Physician Associates scandal? While they can’t stop the next winter crisis, already upon our hospitals?
They announce the intention to fundamentally change Liverpool Women’s Hospital. This was without even a meeting with the organisations that have campaigned for a decade to keep the hospital and collected 75,000 signatures to keep the hospital on the Crown Street site as a women’s hospital for all our mothers, daughters, friends, lovers and for every precious baby.
The whole ICB is facing huge problems and does not have the resources to deliver safe A and E in the coming months. Yet, they think launching a discussion about merging Liverpool Women’s Hospital into one conglomerate of hospitals is sane and responsible.
This is the state of the Integrated Care Board, which is the controlling body for the NHS in Cheshire and Merseyside. It is from page 110 in the Board papers. A score of 20 in black means it is at the highest risk possible. They also said:
“There are currently no known plans for any additional funding to be allocated ahead of winter to support additional capacity and the expectation is that maintaining system flow through winter will need to be achieved through the delivery of these improvement plans.“
The document about Liverpool Women’s Hospital’s future can be found here. We will produce a detailed critique next week.
Maternity and women’s health need urgent changes, but they don’t include dispersing services and absorbing Liverpool Women’s Hospital into one giant conglomerate. We want to see the following changes nationally and locally.
Far better funding and staffing for maternity and an end to birth traumas.
More respect must be given to women giving birth and the women tending them in giving birth.
The funding currently given to insurance for maternity damages should be invested in the service to reduce those damages.
Women who need induction of labour should get that intervention in a safe and timely manner.
Fertility services must be fully available on the NHS, not the prerogative of the well-off.
Gynaecology services must be drastically improved, nationally and locally.
The NHS workforce must be given more respect, their workload improved, and the service must once more become a good place to work.
The whole NHS must be returned to being a national, fully publicly provided service, fully funded, repaired, and restored after all the damages of more than ten years of austerity and many forms of privatisation.
The public’s views must be respected – most women likely to use the hospital will be at work when this first meeting happens.
The research conducted at Liverpool Women’s Hospital must continue into key areas like endometriosis, menopause, and working to ensure our prem babies live and thrive despite being born very early.
Midwifery training must be made available to all without incurring huge debts.
Women’s health and healthcare must be given far more resources and respect.
Our petition, which is available on-line is at 44,656 signatures and more than 30,000 signatures on paper, says “Save the Liverpool Women’s Hospital. No closure. No privatisation. No cuts. No merger. Reorganise the funding structures not the hospital. Our babies and mothers, our sick women, deserve the very best”
It has over seventy-five thousand signatures. The people of Liverpool have attended three big demonstrations to save the hospital. Campaigners have attended every board meeting of Liverpool Women’s Hospital since the petition was launched and every ICB meeting since that was formed. Yet we have never been invited to present our views. Promises of consultation made in public clearly meant nothing.
Twenty thousand signatures were presented to the ICB in January 2023
Liverpool Women’s Hospital is a tertiary centre, which means patients are referred there from other hospitals from the rest of Merseyside and Cheshire, the Isle of Man and parts of Wales. Keeping that provision and the reputation that goes with it is important. The provision for the babies in the neonatal unit, near their mums, matters too.
We have said for years that the NHS must change the maternity tariff, the amount of money paid to hospitals for delivering maternity care. Liverpool Women’s Hospital is the largest provider of maternity care and is badly hit by how low the tariff is. Liverpool Women’s Hospital runs a deficit because of this, and over the years appears to have made some bad decisions on staffing because of the financial problems. Many midwives left. Yet somehow,the document from the ICB says:
“The case for change is focussed solely on the clinical risks, issues and outcomes for people using hospital-based gynaecology and maternity services. It does not consider productivity or value for money.”
The ICB is in serious financial trouble yet it claims not to be considering money in this situation.
We say that right from the beginning, it has been about money. It was about the decision made nearly a decade ago to close one of the Liverpool Hospitals to save money at the cost of our health. It is also about disrespecting women’s health and women’s opinions.
“We’ve known for some time that the poorest households and women have shouldered the greatest burden of austerity measures.” Women’s health has suffered particularly in this time. Liverpool has seen some of the worst overall loss of healthcare. Yet we still kept Liverpool Women’s as a treasured service, where most of Liverpool’s babies are born and where great steps have been made in research. We said before and say it again “In these hard times. what we have we hold.”
Should we leave structural issues in our health care to “the professionals”? No way. The big managers of the NHS have caused havoc in the last ten years, implementing austerity, privatisation, and the move towards an American model. We have seen more than a decade of damage.
Remember the chaos of the building of Liverpool Royal, with fewer beds than the old one and now needing more, with chaos in the financing, construction, and demolition?
We call on the city of Liverpool to defend what we have in the NHS and to fight to improve the rest. No closures, no loss of services, no more mergers, no more outsourcing, no more overworked staff.
This banner in Liverpool Life museum is from one of the campaign groups for women’s health in the early twentieth century
Women and babies in Liverpool are entitled to the highest standard of healthcare. Our grandparents and great grandparents fought to found the NHS and left us this as their legacy. The NHS was a national service providing excellent healthcare, publicly provided and government funded. The new NHS did magnificent work for infant and maternal mortality.
We are campaigning to Save Liverpool Women’s Hospital and to restore and repair the NHS. We want to see improved funding and staffing and to see the whole NHS move back to its original model of a national public service, publicly provided, providing universal comprehensive and timely care for everyone free at the point of need and funded by Government. If you have not yet signed our petition please do so.
Healthcare staff have worked way beyond what should have been needed to keep some good services going. Every day people are grateful for their work, their kindness and humour but sheer human effort cannot compensate for inadequate funding and too few staff.
Liverpool Women’s Hospital provides some excellent services but it has some serious difficulties too.
The Liverpool Women’s Hospital board meeting on 9/05/2024 reported some excellent staff work, including improved methods of helping premature and very premature babies survive and thrive. It also reported the success of moving early pregnancy loss to its own area, a development much valued by the mothers involved. Previous meetings have seen patients reporting their experiences too. In April there was a very positive report from a patient about her experience of the care she received from the Rainbow Clinic as a previously bereaved mum. We have also seen excellent presentations about the pioneering work on endometriosis and menopause at different meetings. The Hospital website says Every day on average, 24 babies are born in Liverpool Women’s Maternity Unit and another three babies are born prematurely and cared for in our Neonatal Unit. Most of Liverpool’s babies are born at Liverpool Women’s Hospital and sick and tiny babies are cared for in the beautiful new NICU ( Neo Natal Intensive Care Unit)
Entrance to the NICU
The Liverpool Women’s Hospital is undertaking a major anti-racism drive to improve outcomes for patients and staff. We very much welcome this initiative. It is essential to save lives.
The core problem for Liverpool Women’s Hospital is under funding. This underfunding stems from the national underfunding of maternity as well as the general under funding of the NHS. This longterm underfunding has meant years of cuts. The NHS organisational changes from 2012 to create Trusts and Foundation Trusts also wasted many resources that should have gone to patient care.
Liverpool Women’s Hospital also has a long waiting list for cancer patients and waiting lists for gynaecology appointments. Some more staff have been appointed and hopefully the list will be dramatically reduced.These waits cost lives and health. The Chief executive reported that
“NHS England’s tiering process for cancer performance is designed to provide accountability and additional central support for trusts that are most at risk of missing national cancer targets. Trusts are categorised into tiers based on their performance, with Tier 1 being the most challenged and requiring the most support. Trusts may move between tiers based on their performance improvements or deteriorations. In a letter received on 26 April 2024 from NHS England, it was confirmed that following a review of cancer performance, and in agreement with the regional team, the Trust will be in Tier 1 for Cancer from the week commencing 29 April 2024. The move to Tier 1 will involve regular meetings to discuss delivery progress and any required support from the relevant parts of NHS England.
Last year the hospital had a poor Care Quality Commission report for maternity and it has taken work to improve on this.New management is in place and they have plans to ensure that improvements are happening.
Our babies, our mothers, deserve much more.Every mother every baby treated at Liverpool women’s deserves the very best. Poverty from low wages, low benefits and poor housing is costing lives, and causing long term ill health. Inadequate health services are part of this.The Care Quality Commision report last year showed how much harm has been done by this underfunding and under staffing. The management must also be responsible for some of the damage mentioned in the Care Quality Commission reports.
The funding issues at Liverpool Women’s means that to meet the current level of service it needs twenty five percent more funding. Money is spent very carefully but for basic safety to be met, that extra spending is essential. At present the required money is being spent and temporary support funding has been made available, by the ICB or national NHS. However this situation puts the hospital into whats called Level 3 of the National Oversight Framework which could bring in management decisions not based on the needs of staff and patients, as the government clamps down on public spending.
Many studies show that money spent on good healthcare repays for itself many times over. At birth this is especially so as bth injuries can last a lifetime.
Neither merging the hospital nor dispersing its services will change that fundamental financial situation. Only an improvement of maternity funding will make a real difference.
The underfunding of maternity leads to staff overwork and reduced services. Government safety figures for staffing are met but we say these safety figures are inadequate. The Government funding does not provide sufficient staff to deliver the kind of service patients and staff require. yet money is squandered on private companies and financial consultants.
There are national problems with maternity services described in many prestigious reports, as well as the Ockendon and Kirkup reports. No report has yet managed to shift the Government’s policies. We believe we need a huge campaign to win back the NHS.
A large part of Liverpool Women’s Hospital Maternity spend is on the maternity Incentive scheme, a government owned insurance system, run on a business model. Liverpool Women’s Hospital meets all the requirements of this scheme and so gets a refund from hospitals that do not meet all the safety requirements. This is an unbelievable situation..
Payouts from the fund are higher than the funding for maternity.If maternity were well funded fewer babies would be damaged and have to claim through the courts from this insurance fund.
In this crazy situation the hospital is still expected to make cuts (CIPs).
Our demonstration last October.
We have written before about how planned Cheshire and Merseyside ICB funding will not repair the situation patients experienced last winter. This poor experience was seen in many aspects, including A and E, care in corridors, access to GPs, access to NHS dentistry, and inadequate mental health provision. It will be worse next winter.
It was no surprise to hear there will be no new Hospital built in the next decade, nor does Liverpool Women’s require a new building. we believe that the new building idea was floated to make the idea of merging Liverpool Women’s Hospital into the big acute hospital more palatable. The existing building is less than thirty years old.However the drive to make fundamental changes remains, with merger or dispersal being the most likely recommendations. WE want to keep a distinct women’s hospital.
In the April Board meeting of Liverpool Women’s Hospital it was reported that work is in progress for major changes.
“the Women’s Hospital Services in Liverpool Programme. As part of the roadmap, the initial phase of the programme had been outlined, with an emphasis on the importance of openness, transparency, and continuous engagement with the public. The development of a clinical case for change was scheduled for the spring and summer of 2024, with publication expected later in the same year. Feedback from this engagement phase, gathered during the winter of 2024/25, would then inform the approach to designing future services, with further development of potential options anticipated to commence in early 2025.” So the threats to Liverpool Women’s Hospital are still very real.
A meeting has been held with other Liverpool hospitals about the future for Liverpool Women’s Hospital and women’s health in the other hospitals in Liverpool.We have not yet been able to see which issues the other hospitals raised. Public consultation is promised this year.
No hospital can exist in a vacuum. Every hospital should be working in a mutually supportive system. The NHS was founded to be a national service, not a collection of competing hospitals. System working was damaged by the 2012 Act and the drive to privatisation. Cooperation and system working is required for the future of the other specialist hospitals in Liverpool, like the Heart and Chest and the Walton Centre.
Our campaign to Save Liverpool Women’s Hospital and to restore and repair the NHS has huge public support and is growing steadily.
For all our sisters,mothers, daughters and babies.