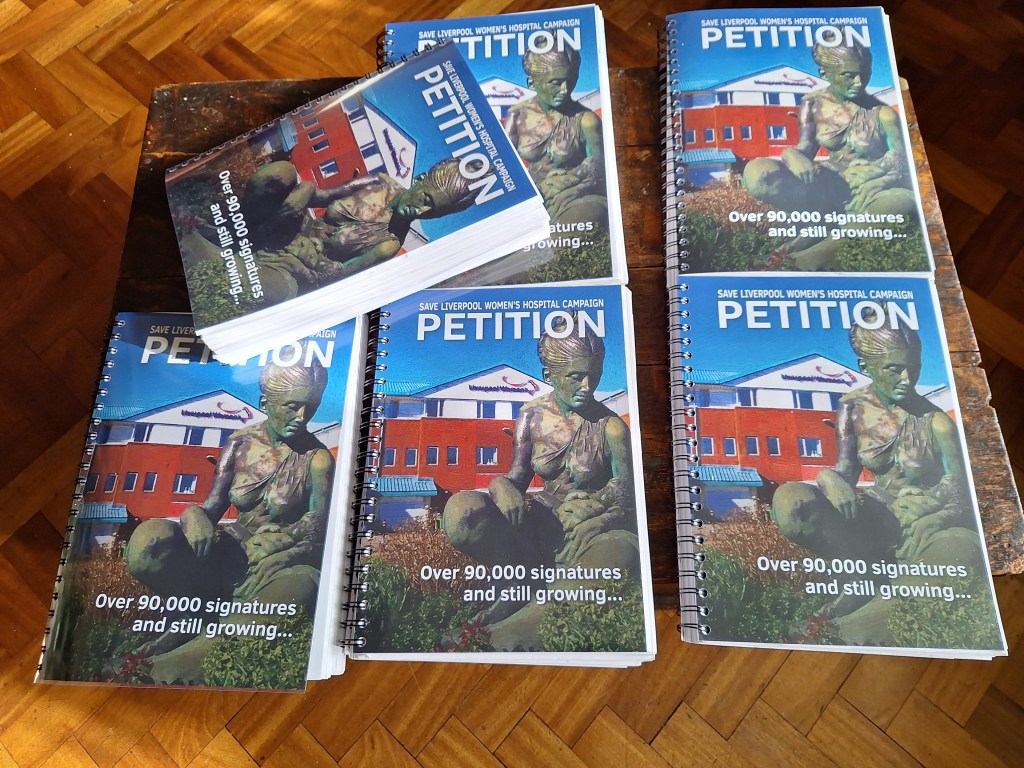
We are campaigning for the best possible healthcare for Women and babies in Liverpool and beyond.The whole of the NHS has been damaged by under funding and privatization. There has been deep disrespect for the people’s health and especially the health of women and babies.The maternity service nationally is scandalously underfunded, understaffed, and under-resourced. Liverpool Women’s Hospital has been under threat all of this time. Our Campaign has fought hard for the NHS and especially for the Women’s Hospital. More than ninety thousand people have signed our petition, both online and on paper. We are still collecting signatures The petition says:
Save the Liverpool Women’s Hospital. No closure. No privatisation. No cuts. No merger. Reorganise the funding structures, not the hospital. Our babies and mothers, our sick women, deserve the very best.
Why is this important? All the maternity and women’s health provision of Liverpool was pulled into this one site. It’s a much-loved hospital. It provides crucial specialised care and the daily joy of new babies. It has a £20 million new neonatal unit and a new diagnostics centre being built. The driving force for closure is a clumsy funding structure, not the needs of women and babies. This is a modern hospital on a good site. and for our mothers, sisters, daughters, wives, lovers, and friends. The alternative wards in the new Royal are not equivalent.
This is a modern hospital on a good site. Our taxes built it for our babies and for our women.
You can see campaigners handing in 20,000 signatures from the petition here.
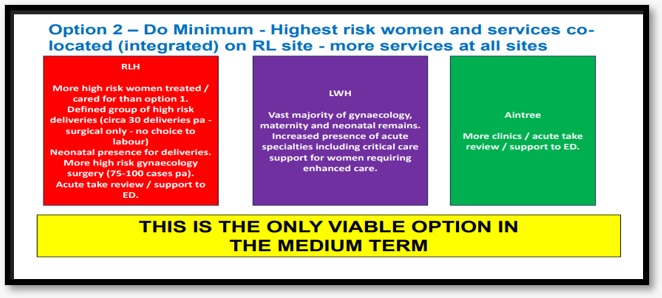
In June and July 2026, the plans for the future of Liverpool Women’s Hospital are out for a public ‘engagement’ exercise. We believe the information being given to the public is inadequate. The process will feature just Option 2. Although a relatively small change, Option 2 is intended to be the forerunner of moving the whole service to the Royal.We say this is unacceptable. These decisions were as plain as the nose on your face at the Cheshire and Merseyside NHS Integrated care Board meeting in January.( The public can attend) These intentions should be made plain to everyone attending the engagement meetings.

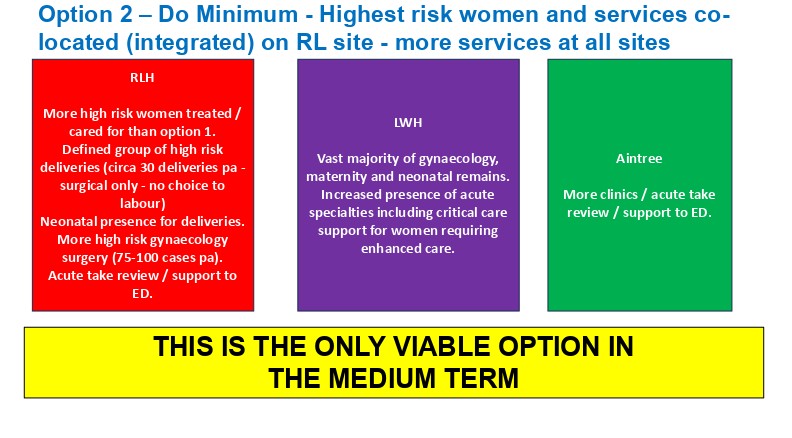
This exercise is part of an intention to, over time, move treatment for women from Crown Street. As we understand it from board papers and attending the ICB, the initial group of women to have treatment under this scheme will be the most complex elective surgical cases in obstetrics and gynecology, who need either immediate access to the highest level of long-term intensive care or joint care from doctors with specialism not included in the Women’s.
Emergency patients are not included and cannot be included. They will still need the specialist doctors. We believe short-term intensive care is available at Liverpool Women’s Hospital. Occasionally, a very ill woman might be best served by ambulance transfer to the Royal or another hospital. The Women’s Hospital reported that they are developing a team for deteriorating patients. We hope this is in place quickly because it is much needed. Meanwhile Option 2 does not address the real issues at Liverpool Women’s Hospital.
How to take part in the Engagement about the future of Liverpool Women’s Hospital

Details of how to take part in this very limited public engagement can be found below, but please read our information on the process too. We believe there are significant omissions in the published case.
If you would like to attend the engagement meetings, they are on.
•Monday 15 June, 2.00pm at Merseyside Fire & Rescue Conference Centre, Bridle Road, Bootle, Sefton, L30 4YD
•Monday 29 June, 11.00am at The Old School House, St John’s Road, Huyton, Knowsley, L36 0UX
• Tuesday 30 June, 5.00pm at Blair Bell Room, Liverpool Women’s Hospital, Crown Street, Toxteth, Liverpool, L8 7SS
This is the registration page link for three public meetings.
Information Sessions – Improving hospital gynaecology and maternity services in Liverpool.
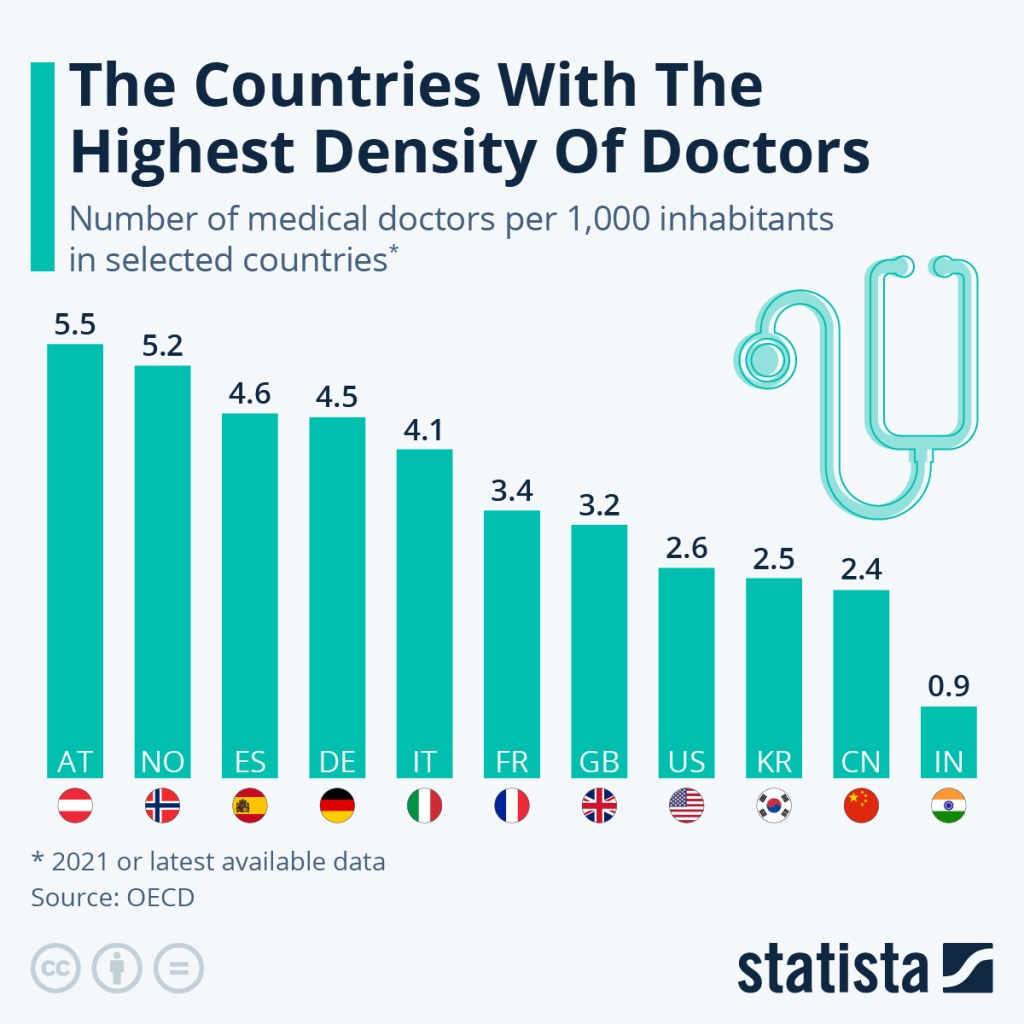
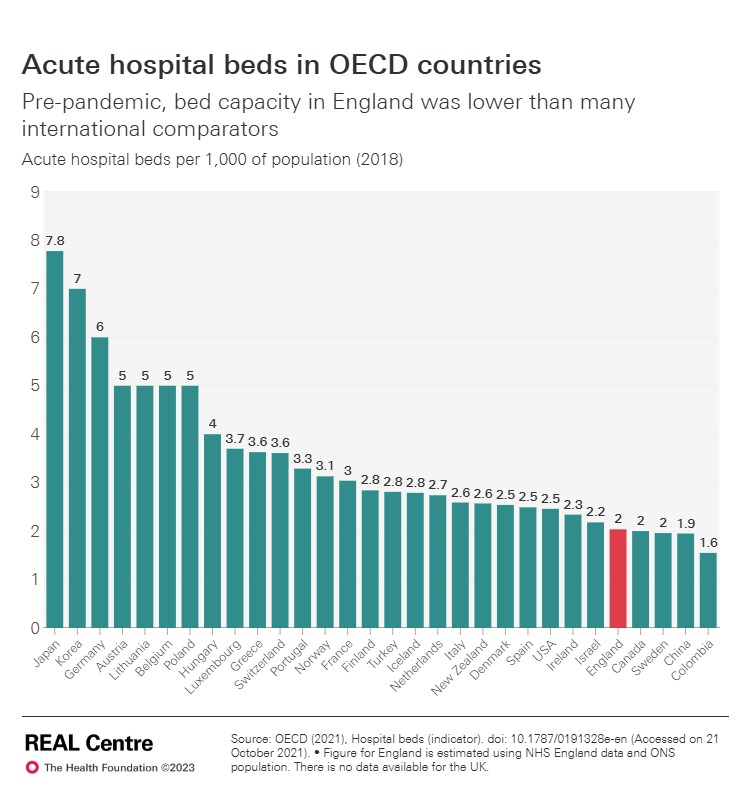
We believe hospitals should work cooperatively, together. The healthcare legislation from Thatcher onward, including the disastrous 2012 Health and Care Act, damaged the natural cooperation between hospitals. Our healthcare has fewer hospital beds per head of population than other advanced countries, fewer doctors per head of population than other countries. To match other countries we would have to hire thousands more doctors. But we have unemployed doctors, The Royal College of General Practice described how qualified G.P.s cannot find posts and the Resident doctors cannot find training posts. This while we need doctors. One in 3 newly qualified midwives cannot find work and other have only part time work. The Independent reported on 4th June 2026 about midwives being told to work double shift with no sleep.
It does not have to be like this. Such madness must stop. Women say No to this nonsense!
Liverpool Royal Hospital, though new and shiny, and with a great staff, has fewer beds than the hospital it replaced. The Royal is overcrowded, as can clearly be seen in the scandalous long trolley waits in A and E, and in the boarding system, not just during the winter.

Some Women’s Hospital services will be dispersed to other places, including some to Aintree. This will mean reduced services Liverpool Women’s Hospital on Crown Street, and considerable extra management requirements to keep track of all the staff and patients in different places.
This will not improve the issues driving the complaints we hear, nor the ones described at the board, which come from lack of staff and resources, failure to heed women and staff raising concerns, and from disrespect for women or medical misogyny, as the government prefer to call it.

The board of Liverpool Women’s Hospital has given its functions to the NHS University Hospitals of Liverpool Group. That is where board decisions are now taken. There was no public consultation on this. It was driven in part by the acute financial problems at Liverpool Women’s Hospital and at the Royal. That board did not mention maternity in its long term plans at the last board meeting. Maternity should be a high priority in any hospital providing that service.
At a recent NHS University Hospitals of Liverpool Board, the figures for building a new hospital for Liverpool Women’s were given as between £350m and £ 500m, and the cost of making the Crown Street site safer was £6 million a year. So it would take 90 years to be cheaper to build.
We believe the information being given to the public in this engagement is inadequate.
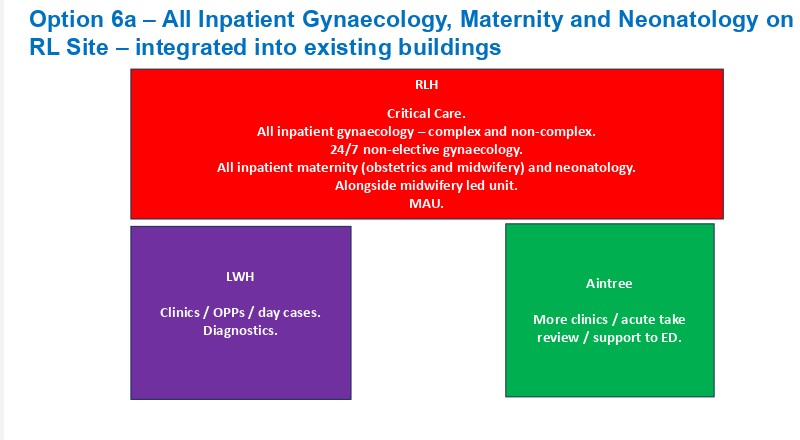
This is not just about some small subset of operations happening at Liverpool Royal Hospital. This is a part of a much larger plan to move Liverpool Women’s services into the Royal.The decisions were made at the January Cheshire and Merseyside NHS Integrated Care Board, the ICB.
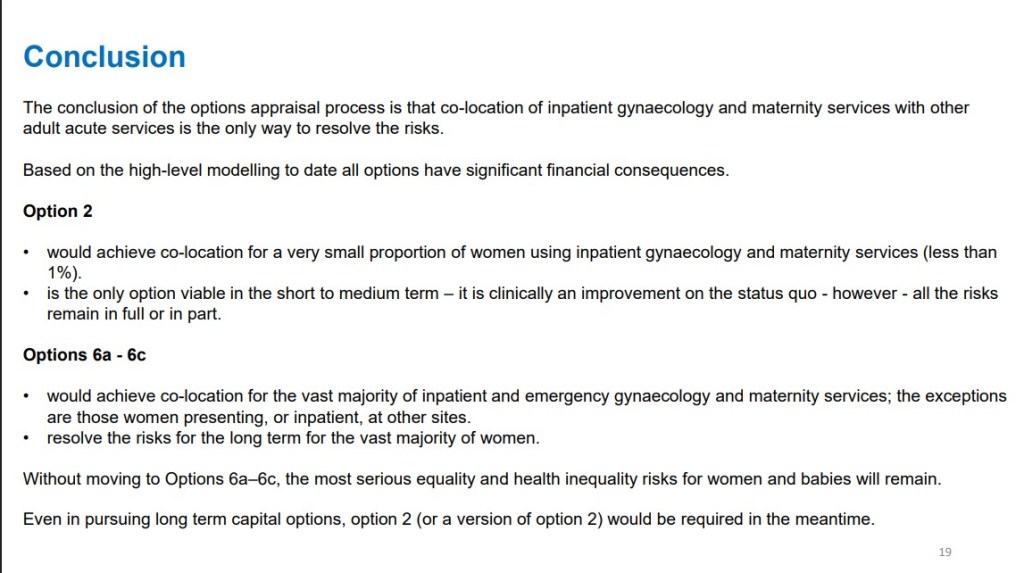
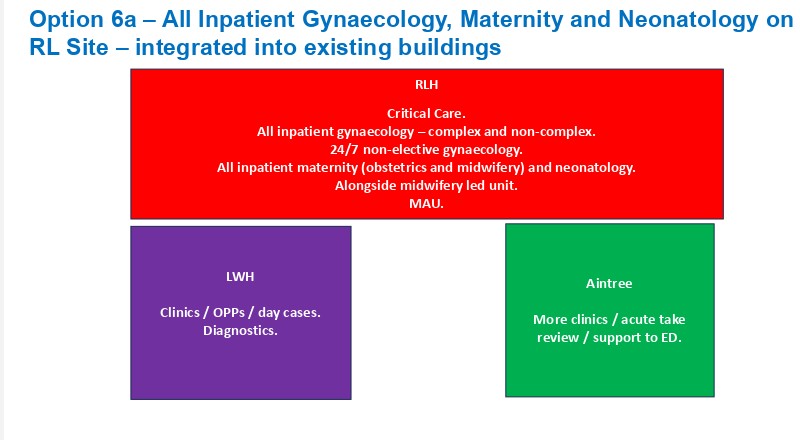
Option 2 is what is being discussed in the engagement process, and bad though that is, Option 6 is the longer-term plan.
The January ICB meeting made it clear (on video 21 minutes -44 minutes in), “…there is no stepping back from the long-term solving of this issue [meaning Option 6] and the need to press the centre and the region for the resource availability and a big capital spend on this…’ ( Sir David Henshaw, the chair of the ICB. This” big capital spend” will compete with other claims on NHS maternity spending.
The public information can be found here: https://www.gynaeandmaternityliverpool.nhs.uk/archives/
The options
We published our thoughts here after the January 2026 meeting of the ICB agreed its plans for the future of Liverpool Women’s Hospital, plans we think are fundamentally wrong and impractical. There is no room at the Royal. We need better funding for Liverpool Women’s and better systems of cross-hospital cooperation.
There have been improvements at Liverpool Women’s Hospital,as reported at the last Group board meeting
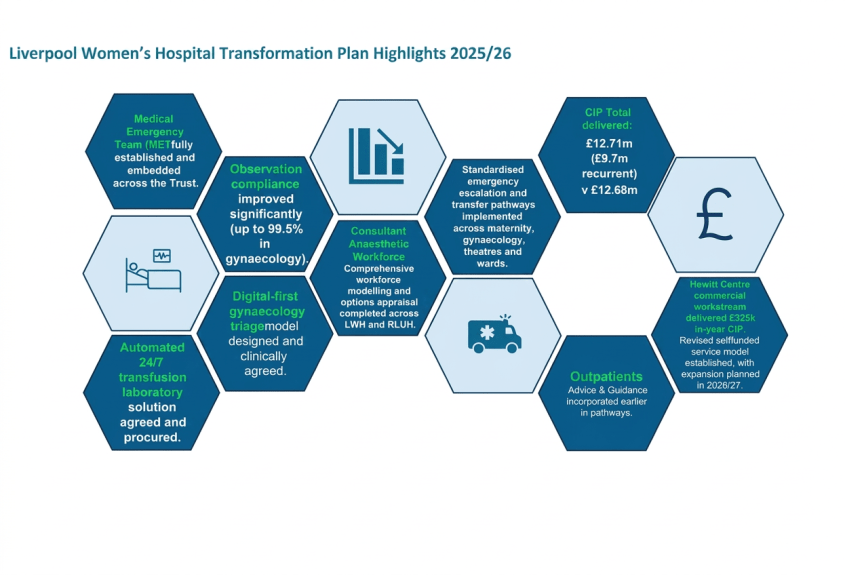
There are also a set of problems at Liverpool Women’ reported at the last Group Board meeting.
” Risk: LWH does not offer the full range of clinical support services required for delivery of complex and tertiary maternity and gynecology services.Cause: Lack of access to clinical support services at Crown Street”
These posts include dietetics, stoma care, occupational therapy, respiratory physiotherapy, dietetics, SALT, pain services and psychology.These are posts that could and should be created. it is not clear exactly why they are not provided at the Women’s but they can and should be so provided. The hospital is in deep financial trouble caused by Government under funding and the particular pressures on Cheshire and Merseyside funding. Other issues have been tackled recently. CIP means Cost Improvement Plans:Cuts to you and me. £12.71 million of them while the hospital lacks some services. The world of NHS cuts is utterly unacceptable
The major maternity crisis in England.
We await two huge reports on the state of maternity care in the UK, one from the redoubtable Donna Ockendon, who has spent two years working on a report from Nottingham. And one from Valerie Amos, who is writing a report for the government. Her interim report was damning. Women want respect in maternity care. The mainstream press is finally picking up what social media and our experiences have been telling us for years. Don’t think for a minute that the politicians and the top NHS bureaucrats didn’t know years ago about the damage going on.
Such is the fear of the state of maternity care that many women are very worried, even avoiding hospital care.
Maternity Buildings are in a poor state.We have a very good building on a good site at Liverpool Women’s Hospital, the Royal is new but not without problems, the Cancer centre is quite new, as is Alder Hey. However the situation in some maternity hospitals is scandalous. Years of Austerity have caused huge damage to the buildings in the NHS.
“Against a backdrop of a £13.8 billion maintenance backlog across the entire NHS estate, over half of organisations reported the formal condition of their maternity and neonatal estate as unsatisfactory, with 42% in need a major repair or replacement and 7% running a serious risk of imminent breakdown.” The Maternity and Neonatal Infrastructure Review Findings report 11th September 2025
Liverpool Women’s Hospital has been affected in the Maternity crisis, with some women, including some of our campaigners, furious over the treatment they received. We are not a fan club for Liverpool Women’s Hospital, nor do we speak for them. We speak for the campaign to Save Liverpool Women’s Hospital. We also have huge admiration for the work of the staff at Liverpool Women’s Hospital, who, despite the difficulties, deliver some excellent service.
We understand they often work with one hand tied behind them due to a lack of resources and management tactics. We are happy to have supported health workers’ picket lines and protests, including the March with Midwives in 2022.
Our Campaign wants Liverpool Women’s Hospital to stay on Crown Street, to be much better funded and much better staffed. We call for it to keep all its services together, on one site (with a better bus service to make the site even more accessible). We want it managed to maximise the health of women and babies. We want all the hospitals to work in cooperation as one health service. But we want to keep the focus on women’s health, and of course, the health of all the dearly loved babies. Splitting the services will cause damage to those services and grief and annoying inconvenience for years to come. Imagine some clinics being at Crown Street, some at Aintree, some at the Royal, and some, God knows where. Imagine navigating that with a baby and a toddler.
Far Worse than inconvenience and thereby missed appointments, there is a very real danger of women’s health issues being further minimised and ignored. That is what has been happening in the NHS (and in other countries that have adopted austerity as policy) for the last twenty years, and these problems have been centred in the big, merged hospitals. The reports of major scandals being investigated by Valarie Amos are in the big hospitals. Leeds and Shrewsbury were removed from the list because of other ongoing enquiries. The 14 NHS trusts are:
- Barking, Havering and Redbridge University Hospitals NHS Trust
- Blackpool Teaching Hospitals NHS Foundation Trust
- Bradford Teaching Hospitals Foundation NHS Trust
- East Kent Hospitals Foundation NHS Trust
- Gloucestershire Hospitals Foundation NHS Trust
- Leeds Teaching Hospitals NHS Trust
- Oxford University Hospital NHS Foundation Trust
- Sandwell and West Birmingham Hospitals NHS Trust
- The Shrewsbury and Telford Hospital NHS Trust
- The Queen Elizabeth Hospital, King’s Lynn NHS Foundation Trust
- University Hospitals of Leicester NHS Trust
- University Hospitals of Morecambe Bay NHS Foundation Trust
- University Hospitals Sussex NHS Foundation Trust
- Somerset NHS Foundation Trust
The worst-off women, and those from Black, Asian, Gypsy-Romany and Traveller backgrounds, have been most damaged in this Maternity crisis. Please see our earlier posts.
Liverpool Women’s Hospital is at the heart of Liverpool 8 and much loved there. It seems very bad to be damaging Liverpool Women’s Hospital just as these reports are due to be published. A large public meeting chaired by Kim Johnson MP made the opinions of local people very clear.
Liverpool Women’s Hospital is well-loved.
The women of Liverpool have loved the Liverpool Women’s Hospital since it opened, and they loved the previous women’s spaces like Catherine Street and Mill Road. Far too many women experience domestic and sexual violence and are aware, in brain and instinct, of the need for a safe space, organised by and for women, when they are at their most vulnerable. But it’s not just violence – medical misogyny plays a role too.
This love of the Women’s Hospital has a scientific base. The NHS has truly ignored women’s health.
“Women’s bodies have been treated as medical mysteries, not because they are complex, but because they have been excluded. From research funding to clinical trials, a gender data gap runs deep through modern medicine, shaping who gets believed, who gets diagnosed, and who gets left behind.
Less than 2.5% of medical research funding goes to women’s reproductive health – despite women and girls making up more than half the world’s population 1 .
This imbalance is not an accident; it reflects a pattern of medical misogyny, a system that undervalues, underfunds, and misunderstands women’s health.
The consequences are devastating. Women are being dismissed, misdiagnosed, or left in pain for years before receiving answers. Many turn to online communities for help after being told by doctors that their symptoms are “normal”, that they are “making a fuss about nothing”. For people with endometriosis, the average diagnosis time is nearly nine years. Nine years of pain, endless appointments, and disbelief.”
It’s vitally important to keep a women’s space. Not just a physical space, but a place of science and care devoted to women and their babies. A space with a well-qualified and well-treated workforce focusing on women’s health, where women are heeded as women and not dismissed. There is a quiet but fierce rage behind the demands for a woman’s place in healthcare.

No one can deny that the fashion for huge hospitals has at least coincided with real drops in the quality of maternity care and long waiting lists for Gynaecology. These mergers started in the 1990s with the policy of making hospitals work like competing businesses, and then a second wave in 2010 with the Foundation Trust era, as smaller hospitals were pushed into mergers by a financing model that favoured the big hospitals This at least coincided with the deterioration of Women’s health care. Women’s health has indeed deteriorated.
Parliament’s Women’s Equality Committee ( these are MPs, not the government) has twice described the situation for women in great detail but has not been able to secure the necessary funding to improve matters. The first WEC report stated that ‘Medical misogyny’ is leaving women in unnecessary pain and undiagnosed for years”.
We also recognise the importance of the physical environment, and Liverpool Women’s is one of the best hospitals in that respect.
Austerity and political misogyny have a lot to do with the neglect of, and damage to, women’s health. The NHS has been underfunded and consequently understaffed for the years of Austerity, and the future is looking grim too. In 2025-6 and 2026-7, the cuts imposed in Cheshire and Merseyside NHS and through them to the Hospitals and out-of-hospital care are awful. For more details, see this.
Hospitals are under huge financial and political pressure. See Liverpool Women’s Hospital in the Eye, The NHS Storms, written earlier this year.
Women’s health and healthcare in the NHS
Women in England have a life expectancy of about 83 years, but their Healthy Life Expectancy (HLE) is roughly 61.9 years. This means women live upwards of 20 years in ill health.
This is worse in areas where people are struggling with the cost of living, and worse for women with high caring responsibilities, like much of Liverpool, especially where the cost of living is hitting hardest.
And;
“One key point is how females and males differ in many biological and social factors that fluctuate and, sometimes, accumulate over time, resulting in them experiencing health and disease differently at each stage of life and across world regions. The challenge now is to design, implement and evaluate sex- and gender-informed ways of preventing and treating the major causes of morbidity and premature mortality from an early age and across diverse populations.”
The NHS has not done such a good job in the big general hospitals in achieving that understanding, nor in establishing good practice, so there remains a good case for a women’s hospital.
“What happens in pregnancy and early childhood impacts on physical and emotional health all the way through to adulthood the UK dropped from 20th to 26th place (out of 38) in the Organisation for Economic Cooperation and Development (OECD) on female life expectancy between 2000 and 2022. This compares with a drop from 14th to 19th place for male life expectancy during the same period healthy life expectancy among women fell by 2.5 years between 2019 to 2021 and 2022 to 2024”.
Heart and Cancer, too, have neglected women.

It’s not just in the exclusively female aspects of medicine that we see neglect of women. It is true in heart and cancer, too.
There is much written and studied about women and heart disease.
“Recent data published by Professor Chris Gale from the University of Leeds, funded by the British Heart Foundation, found that more than 8,200 women in England and Wales could have survived their heart attacks had they simply been given the same quality of treatment as men, according to their paper in the journal Heart. The researchers found that women in the UK had more than double the rate of death in the 30 days following their heart attack than men. The researchers suggest that this may be, in part, explained by women being less likely to receive guideline-recommended care.”
Some heart/cardiovascular diseases are exclusive to women and linked to their reproductive health. The improvements must come from all sectors of the NHS.
Women have different heart attack symptoms from men, and it helps if we know these symptoms. It helps if the NHS remembers them too!
Cancer
Several years of National Cancer Patient Experience Survey data shows that women are less likely to be treated with dignity and respect and less able to discuss their worries when receiving hospital care than men – an indictment of NHS culture. The NHS’s inability to listen, itsreluctance to give patients meaningfulpower and choice, and its tendency to disempower patients despite them being the real experts in their own health conditions, is ‘by design’.
They also say, “That is to say, it is a feature of a care model that is:
• one size fits all
• too focused on provider interests, rather than patient interests
• highly paternalistic, centralised and bureaucratic”
The NHS gets a pasting in these reports, but we think something big is missing from the reports.
NHS staff have faced obstacles in getting the resources they need to treat people as they should be treated . Years of cuts, privatisation, and meddling with NHS structure have caused huge damage, and the staff carry no blame for that. Rather, they have worked against the odds to maintain the service.
Lord Darzi, who produced a report about the NHS immediately after the General Election, said, “The Health and Social Care Act of 2012 was a calamity without international precedent. It proved disastrous.” We think the Health and Social Care Act 2022 was another disaster, and Wes Streeting’s sweeping attacks on NHSE and the ICBs have caused another wave of disruption.
We support the original NHS model. This was a universal healthcare service, free at the point of need and paid for by the government. It was a national service with all parts cooperating, but with strong local involvement. Investing in health care makes the economy stronger, not weaker, and helps the population’s health and happiness. Even the right-wing World Bank says so. The wave of privatisation and for-profit companies being involved in the NHS has been an utter failure for patients and staff.
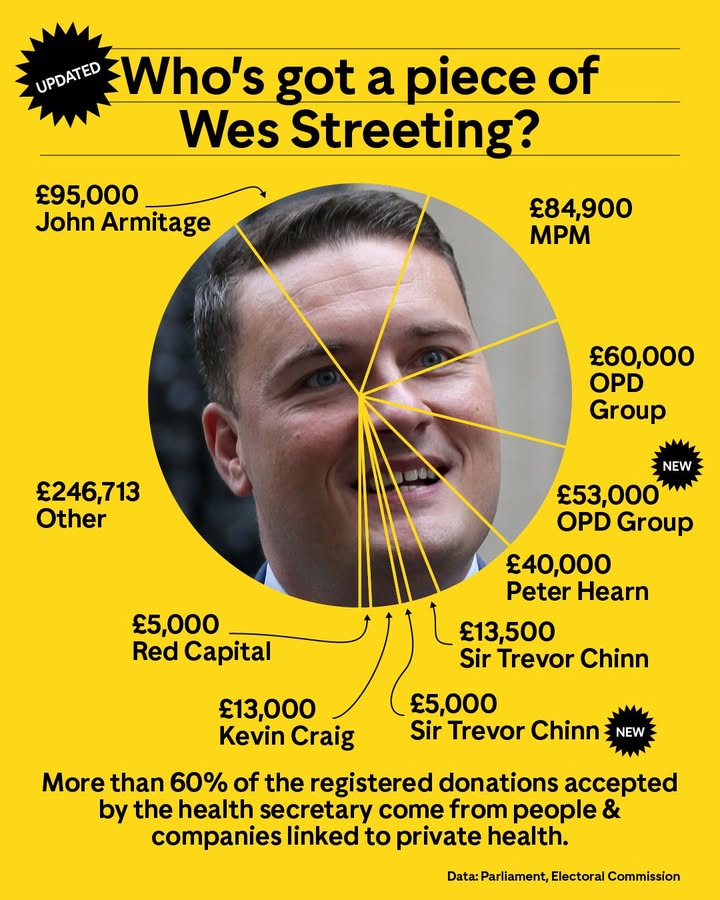
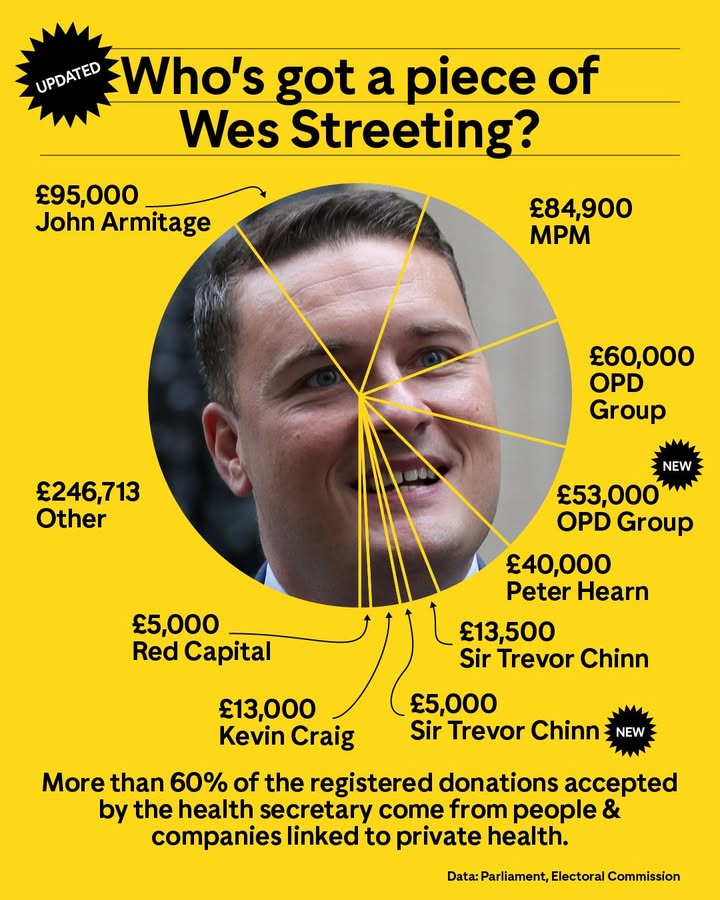
It is a crying shame that Labour politicians, including the not lamented Health Secretary Streeting, have taken money from those who make big profits from healthcare.
The situation in Liverpool is especially serious. In the document Health in Liverpool 2040, it was made clear that the health of women in Liverpool is declining.
“In Liverpool, women can expect to live 57.9 years in good health, and men up to 58.3 years-this means on average women will spend 28% of their lives in poor health, whilst men will spend 23% poorly.
For women, healthy life expectancy is lower than at the turn of the decade, and the gap with England has widened from 5.5 years to 6 years, while for men, the gap continues to be 4.8 years.
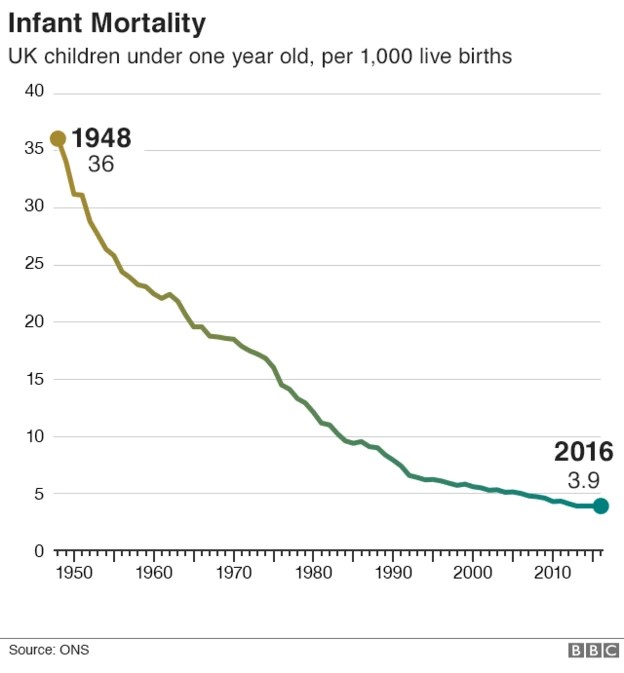
“The infant mortality rate has long been regarded as a key indicator of population health that is sensitive to the prevailing socioeconomic circumstances affecting children. In Liverpool, around 26 infants every year do not reach their first birthday.”
“What happens in pregnancy and early childhood impacts on physical and emotional health all the way through to adulthood”
All of this supports a focus on women’s and children’s health, needs currently not being met nationally or locally. This in not to the detriment of men, but because women have different needs
“As we go marching, marching, we battle too for men, for they are women’s children and we mother them again.”
Women also experience sexual and domestic violence, poverty through low wages and inadequate childcare. It takes two incomes to raise a family. Hospitals can only contribute about one-third of what is needed for good health for women. Good affordable food, good housing, clean air, low stress, well-paid jobs, confidence in the future, freedom from assault all help our health outside hospital. But when we as women come into the hospital, it is because we need help. That help must be skilled, respectful, compassionate and well funded.
Too Many Hospitals in Liverpool ?
The NHS seems to believe that there are too many hospitals in Liverpool; they have done for years. The history of this was covered in a Post article called “https://www.livpost.co.uk/a-fucking-feudal-baron-the-long-legacy-of-liverpools-most-feared-nhs-boss/ The article says that a fan of Mrs Thatcher running the local NHS in the 1980s pushed through all the hospitals in Liverpool becoming Foundation Trusts. Liverpool has a different pattern of hospital care from many other cities, and the government wants to change that. It is pushing the ICBs and Hospitals to make drastic cuts.
In 2014, there was a Panorama programme saying that Liverpool has too many hospitals. The next day, it was announced in the Echo that Liverpool Women’s was the hospital that would close.
We started our petition, at first online and then on paper, and we have fought for many years to keep the hospital open.
The process of merging the hospital is underway.
The board-level management of Liverpool Women’s Hospital has been handed, without public consultation, to the University Hospitals of Liverpool Group. However, the Chief Executive of that group has resigned. This coincided with plans to take all Liverpool Hospitals into that group being knocked back nationally. The public now has much less chance to monitor what goes on in Liverpool Women’s Hospital. Board papers cover all the hospitals, There have been major changes in the senior staff. There is no one on the board with a record of work in maternity, nor in Gynecology. The recent long-term plan, discussed in the May meeting of the hospital group, did not even mention maternity or women’s health.
We all have good reasons to be concerned.