If you joined our protest on September 28th in Liverpool (or wished you could have done so), thank you. You are invited to stay in touch to develop ongoing campaigns, to convince others that we can win back the NHS, build understanding and determination, and work together to build a movement so significant that no government can ignore us. Maternity and women’s health have been damaged for many years. We say “Enough is Enough. Restore, Repair and Rebuild the NHS. Repair and rebuild the maternity services and gynaecology care”
We say, as Christabel Pankhurst, one of the suffragettes, said, ” Remember the dignity of your womanhood. Do not appeal, do not beg, do not grovel. Take courage, join hands, stand besides us, fight with us.”
Bread and Roses, the song of women’s struggles, says”As we come marching, marching, we battle, too, for men— For they are women’s children and we mother them again”
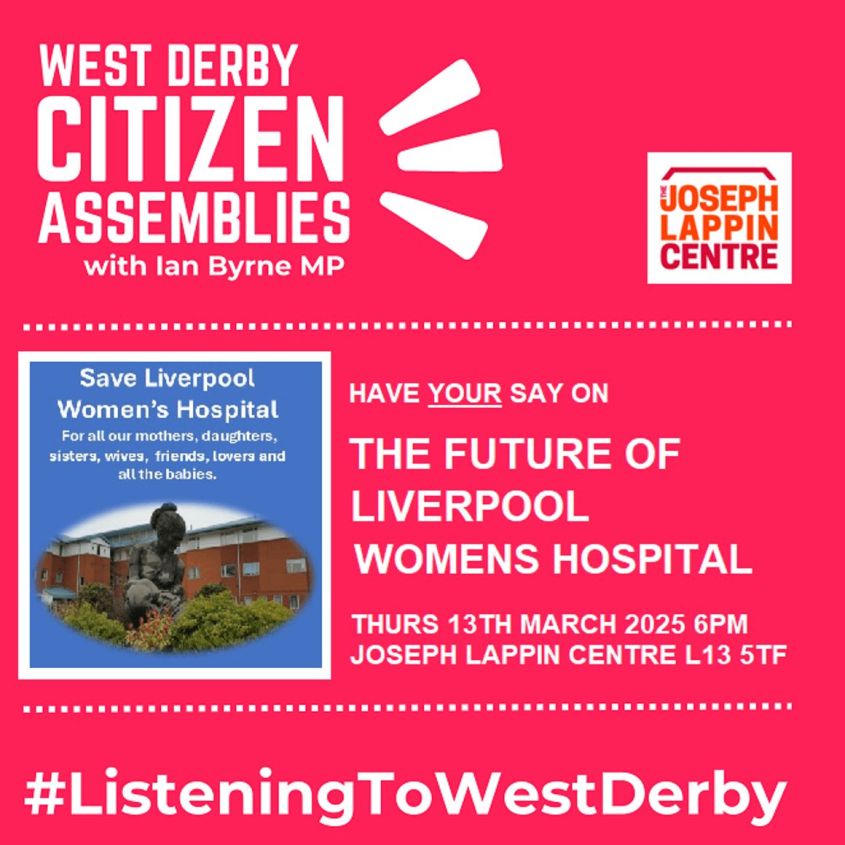
Maternity and gynaecology remain a key focus for the Save Liverpool Women’s Hospital Campaign. Please refer to our other posts for more information on this topic.

Working together, experienced and new campaigners, we can gather experiences from the NHS, including those of patients, staff, unions, families, communities, and campaigns.
We each care about the NHS for our own reasons. Some because the NHS has saved their lives or loved ones’ lives, some because of the failures in the NHS, and some because they can see that things could be so much better.
You can and should be allowed a say in how the country organises healthcare. The big corporations that are trying to privatise it don’t want us to have a say, but that’s no reason to be silenced.
We are campaigning for just and effective health economics, as well as the politics of health. This is not the same as practising medicine or providing individual healthcare. That requires qualified professionals, but those professionals are not the arbiters of how a country organises its healthcare. That is a political decision, one to be made, in a democracy, by the people.
Even the World Bank says, “Investing in health is one of the most powerful drivers of economic growth and job creation“.
Modern cities require both public health measures and healthcare for their residents.
Without good public health systems, terrible illnesses rip through the population, as happened in 19th-century London, where even Prince Albert, the husband of Queen Victoria, died of typhoid. Other diseases like Cholera and tuberculosis, smallpox and scarlet fever attacked some of the rich as well as many of the poor. Providing healthcare only for the rich did not protect even the rich. A system of universal healthcare is necessary.
This blog discusses how the UK’s healthcare system is being damaged and how to restore, repair, and rebuild it. It is essential to note that poor housing, polluted air, inadequate food, poorly heated homes with damp and mould, and traffic pollution, as well as a lack of access to green spaces and workplace dangers, including stress and low wages ( the social determinants of health), all contribute to illnesses. We support campaigns for good housing, good food, cleaner air, and decent childcare.
Countries choose from different forms of healthcare. A very few countries leave it to people’s ability to pay and let the rest go hang, much like the UK before the NHS was established. They are mainly in very poor or war-torn countries. Before austerity, the World Bank and other international institutions imposed “structural adjustment” on poorer countries, which damaged healthcare and education. The damage is serious. The UK was severely damaged by Austerity, as other countries had been damaged previously by structural adjustment. This was a political decision of the government. The UK had a choice in this that was not shared by poorer nations
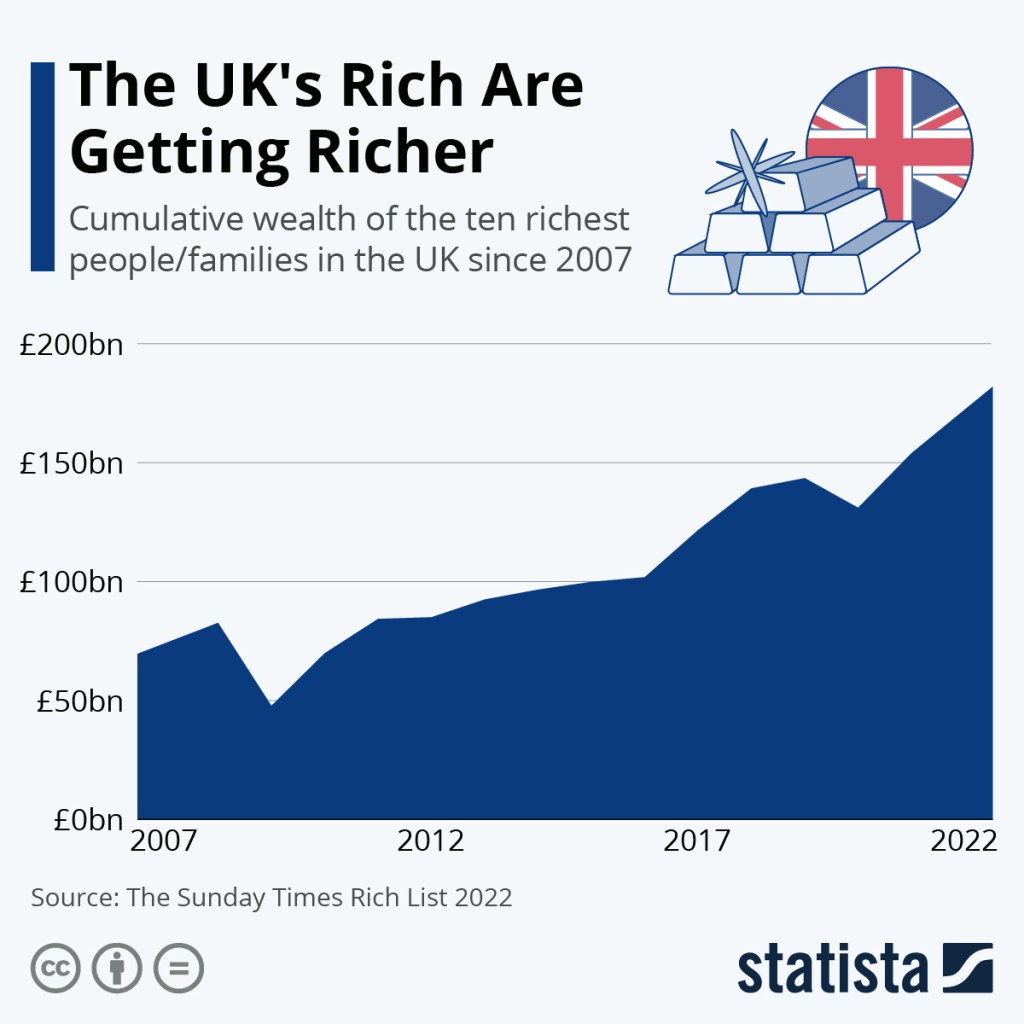
The UK, was the economy hardest hit by Austerity, and it was the poor that were hit, not the rich; “Overall, austerity measures resulted in about 190,000 excess deaths, or a 3% increase in mortality rates, from 2010 to 2019, including many ‘deaths of despair‘.”
“The world is off track to make significant progress towards universal health coverage (Sustainable Development Goals (SDGs) target 3.8) by 2030. Improvements to health services coverage have stagnated since 2015, and the proportion of the population that faced catastrophic levels of out-of-pocket health spending has increased continuously since 2000. This global pattern is consistent across all regions and the majority of countries.”
So political decisions directly affect healthcare.
Health care systems are essential in urban culture, where people live close together and share water sources and drains, as diseases spread too easily.
Some countries (not many) have a fully commercial model of healthcare designed for profit. Because this cannot be easily implemented in an urban environment, the government has to step in and subsidise it for certain groups of people. ( mainly the poor) Some are still left outside the safety net. The USA uses this model of healthcare. It is a cruel and costly model, but highly profitable. It is the system from which many advisers to our Government come; companies involved in the US system are deeply involved in ours. These corporations are exploiting the money that voters think is going to our healthcare. It should not be going to profit.
The US government pays significantly more per person for healthcare than the UK pays per person, and its people don’t all receive coverage; they must also pay for insurance in addition to the government’s contribution. Much of what the US government spends on healthcare does not go to patient care, but rather to insurance companies or healthcare corporations. The NHS model is the most cost-effective, but it generates less profit for large health corporations.
Some countries (like France) have compulsory health insurance with co-pays. Co-pays are where the patient bears some of the treatment costs, and the insurance company covers the rest. This system too has its own problems. It does provide universal coverage; everyone can, in theory, access healthcare, and the nation’s health is good.
Ireland has a complex mix of charges and insurance. People can get some of the fees they have to pay back from the government. Ireland has some excellent outcomes in its health care. “Life expectancy at birth in Ireland was higher than the EU average in 2021, at 82.4 years”
These mixed systems are costly to both individual people and the government.
Even in France’s system, people are employed to administer the insurance and verify it against the hospital charges. Insurance companies and hospitals require numerous administrators. This is money that could be directed to patient care and is, in fact, so directed in the original NHS system.

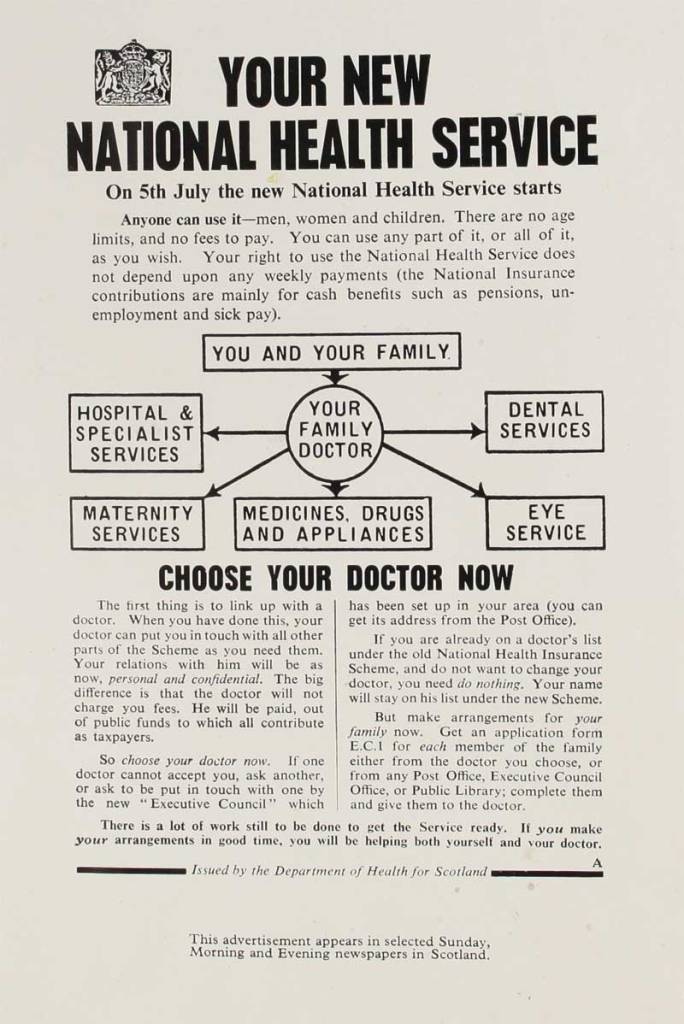
The UK in 1948 chose the universal public service model on which the NHS is founded. We campaign for a return to the original NHS model. This model is both cost-effective and efficient, and it allowed the system to be recognised as the best in the world in 2014. Since then, privatisation, along with the introduction of a business model, competition and cuts, has seriously damaged our healthcare.
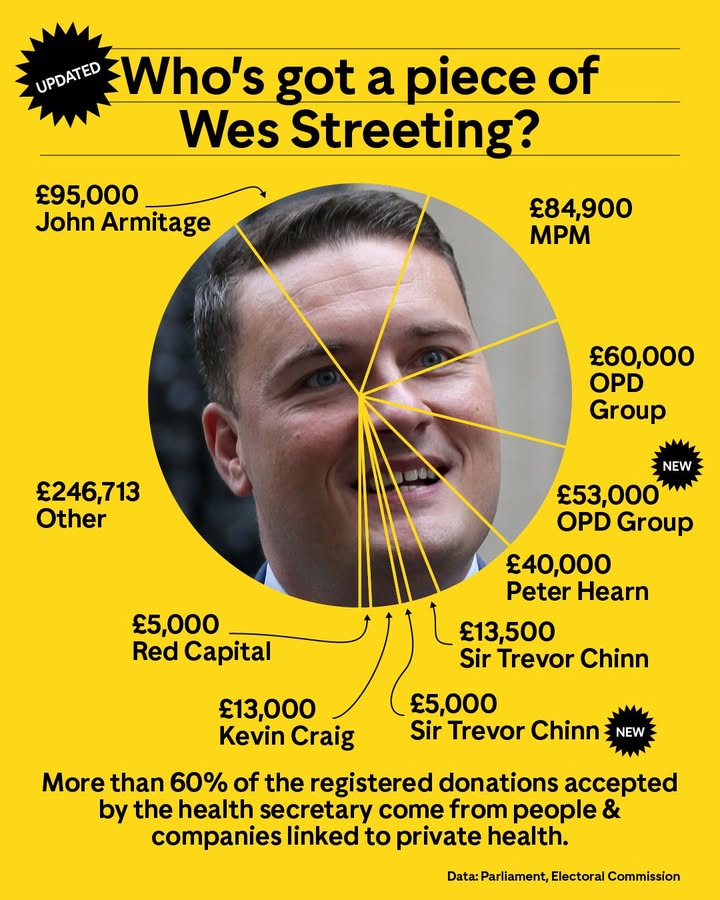
“Employees, lobbyists, and consultants secure advisory or leadership roles in government bodies and then move back to the private sector. Meanwhile, senior government officials and former ministers take their inside knowledge and contacts to organisations and sectors that do regular business with government.“
The damage to healthcare in the UK during the years of austerity, privatisation, and the ICB system is very well described here by Deborah Harrington from Public Matters. Deborah is a long-term supporter of our campaign.
Please do get involved or continue to be involved. We can win this, but it will necessarily require the involvement of thousands of ordinary people.
There are many different but linked NHS campaigns. Please contact any organisation you might like to work with, and get involved.
Save Liverpool Women’s Hospital; email us at savelwh@outlook.com or reply to this blog post.
https://keepournhspublic.com/about-us/
http://www.thepeoplesassembly.org.uk
Many trade unions work hard on the issues around the NHS, but would welcome activists to do more. Please contact us if you would like to learn more.


Getting more involved can be:
*learning more, sharing your knowledge, or experience,
*talking to people about the NHS
*helping get information out to others,
* organising events, working together to get communities interested,
*getting people interested in the workplace,
*making it clear to politicians that we won’t tolerate unnecessary deaths and suffering any longer.
So, what will the Save Liverpool Women’s Hospital Campaign be doing, opposing or protecting, in the months to come?
• Campaigning to save Liverpool Women’s Hospital and exposing the extent of the national Maternity crisis. For more information, please refer to our other blog posts.
*Campaigning against the Winter Crisis. The winter crisis is going to be grim, as people are already kept on trolleys in corridors for days. We must build the protests about this. Last winter, delays in treatment in unsuitable situations resulted in many lives being needlessly lost.
*Staff shortages and the pressure on hospitals to make redundancies.
*The ongoing plans to bring more American-style privatisation into the NHS.
Ordinary people must begin to discuss the running of the NHS as if it were indeed their business, and their right. We must remember how we won the NHS and apply those same campaign tactics to win it back.

What would it look like to restore the NHS?
People would be able to get good healthcare more easily.
Migrant charges, which cost so much to implement and bring in less than they cost, would be abolished.
The NHS would once again be a national public service, publicly owned and delivered by people employed in that service. It would be based on cooperation, not competition, between different hospitals.
This model of healthcare provision is much less expensive for the government than the American model. Yes, the American system, where people have to pay huge healthcare premiums, still costs the US government twice as much per person as the NHS costs.
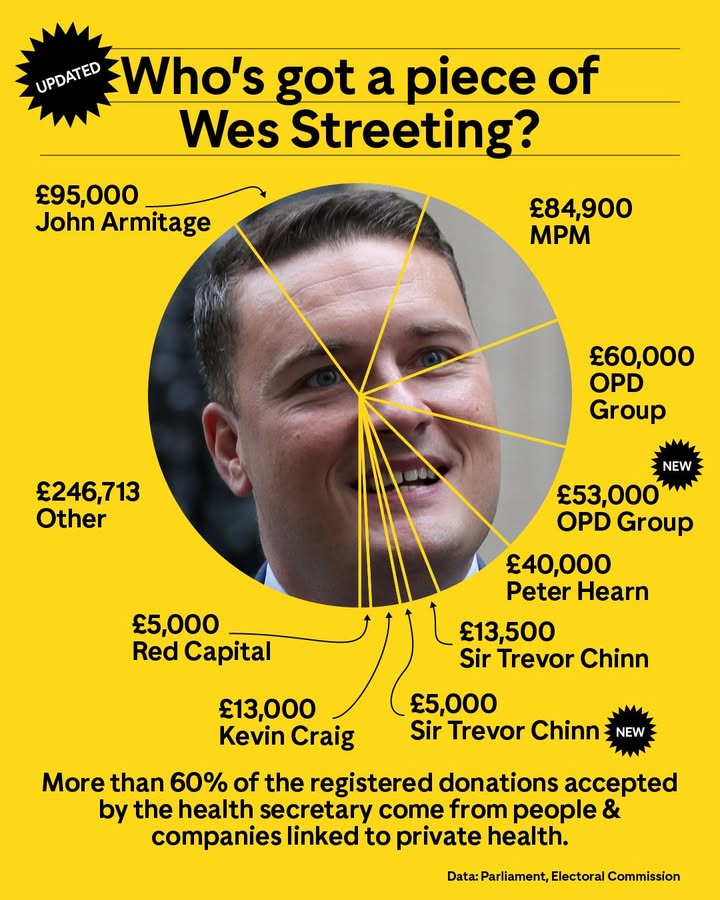
If the NHS were restored, all the privatisation introduced by the 2012 and 2022 Health and Social Care Acts would be reversed. No outsourcing, no privatisation, no use of US models of companies making a profit from our healthcare, no more big US corporations advising on how to run the NHS. No more donations to politicians from private health companies. No more movement of key people between lobbying, working for the private health sector and working in the NHS.
No more substitution of less qualified staff for highly trained professionals.
It would go back to the founding principles of the NHS. Those principles are;
Keep Our NHS Public also wrote that the founding principles included
The NHS as a comprehensive service, universally available, based on clinical need, free at the point of need, and funded through collective contributions.
◼︎that it should be comprehensive – meet the needs of everyone;
◼︎that it should be universal – free to all at the point of delivery to access GP consultations or hospital treatment;
◼︎and that it be based on clinical need, not ability to pay.
We would add that, over the years, building a highly educated and reasonably well-paid workforce was a core part of the NHS. Now, many hospitals do not even pay the living wage, and qualified doctors have no post; nursing and midwifery students are graduating with no jobs to go to (there has been some movement from the government on this, but not a satisfactory resolution).
Campaigns do have an effect. Women got the Vote, we got the NHS, we got equal pay for equal work, we won abortion rights, we stopped the poll tax, and more, all from campaigns and through working together.
It is vital that more people feel confident discussing the NHS with their friends, family, and workmates. It’s very common in the US to discuss the healthcare system; we also need to discuss our system, not just the damage it has sustained. We don’t have to be doctors, nurses, or midwives; we just have to be people.
What would it mean if the NHS were repaired?
Then funding would be improved, and waste that now occurs through privatisation would be redirected into front-line care.
We would begin to recruit enough doctors, nurses, midwives, other health professionals, and ancillary staff to levels that at least match those of other wealthy European countries.
We would have many more hospital beds.
Staff and patients would have more say in the running of the services.
GP services and the entire Primary Care service would be improved.
Public health services would be improved; The Lancet reported that “Public health grant allocations in England have been cut by 24% in real terms per capita between 2015–16 and 2021–22.”
Staff working conditions would be improved, and workload pressures would be eased.