Take the fight for the NHS to the communities and workplaces!
The NHS originated from working-class organisations, including unions, and crucially, among working-class communities, especially among working-class women. We have records of this on Merseyside.
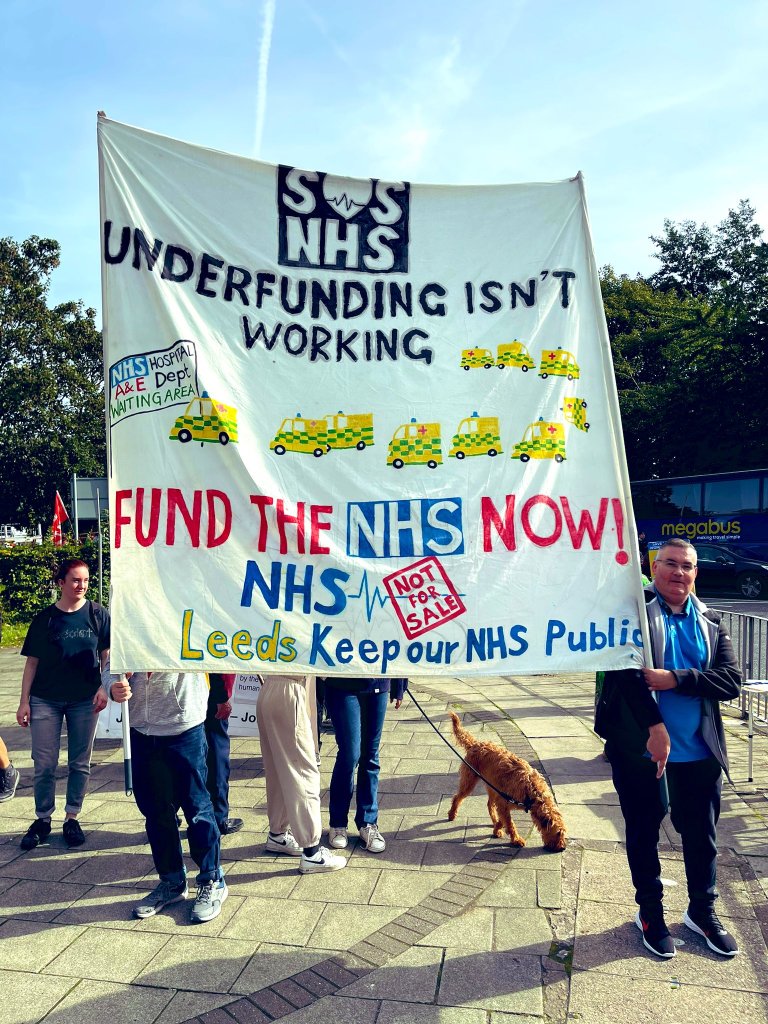
Talk about the NHS with friends, family and people at work. Work with other campaigners to get the word out to communities through leaflets, stalls, research, public meetings, pickets, posters, conferences, and demonstrations. The NHS is ours, a legacy from the generation that defeated fascism and built the welfare state. Stop the daylight robbery of this service by huge corporations.
Help us lobby the ICB (the governing body of the NHS in Cheshire and Merseyside; there are similar organisations across the country). They are based on the US system of Accountable Care Organisations, designed for privatisation and profit-taking, denial of care, extracting charges from patients and downskilling of staff.
We are working on model resolutions to restore, repair, and rebuild the NHS, so you can move them at union branches (for unions that are not currently organising NHS workers). Your suggestions are most welcome.
We are building links with health service workers, but help with this would be most welcome.
We ask that political parties that do support a return to the Bevan model of healthcare ensure their political education and campaigning include the campaign to restore the NHS.
When the Labour Government in 1945 decided to set up the NHS, the core principles were clear.
Healthcare for all, free at the point of need.
A national universal service cooperating across the country.
A service which is funded as a public service and delivered by a publicly owned and controlled service.
A service that is a good employer employing fully qualified staff, which pays good wages and has manageable workloads without driving burnout.
We would add
Remove all privatisation.
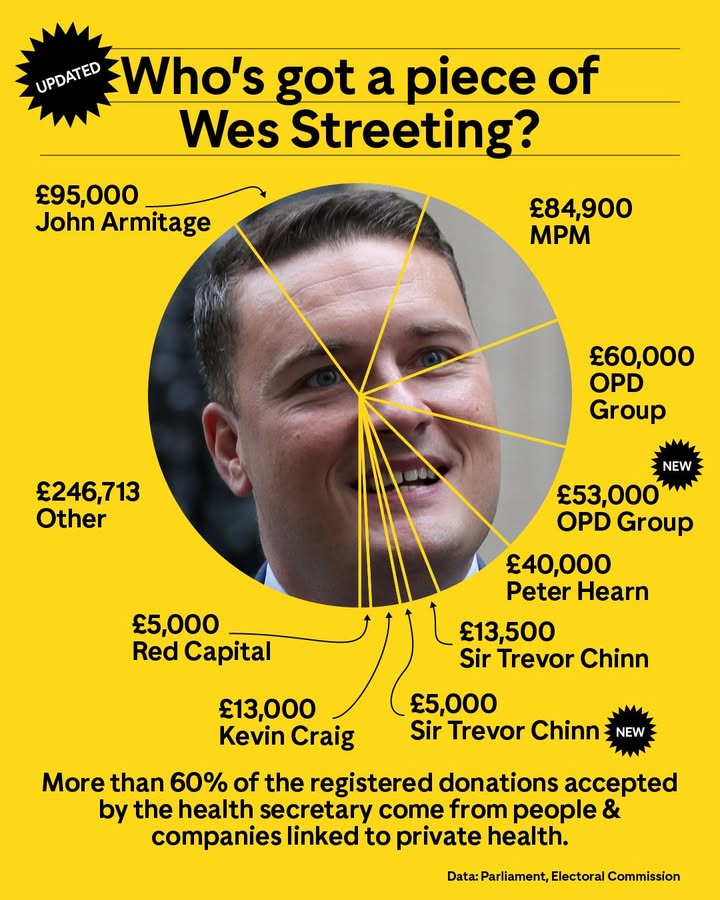
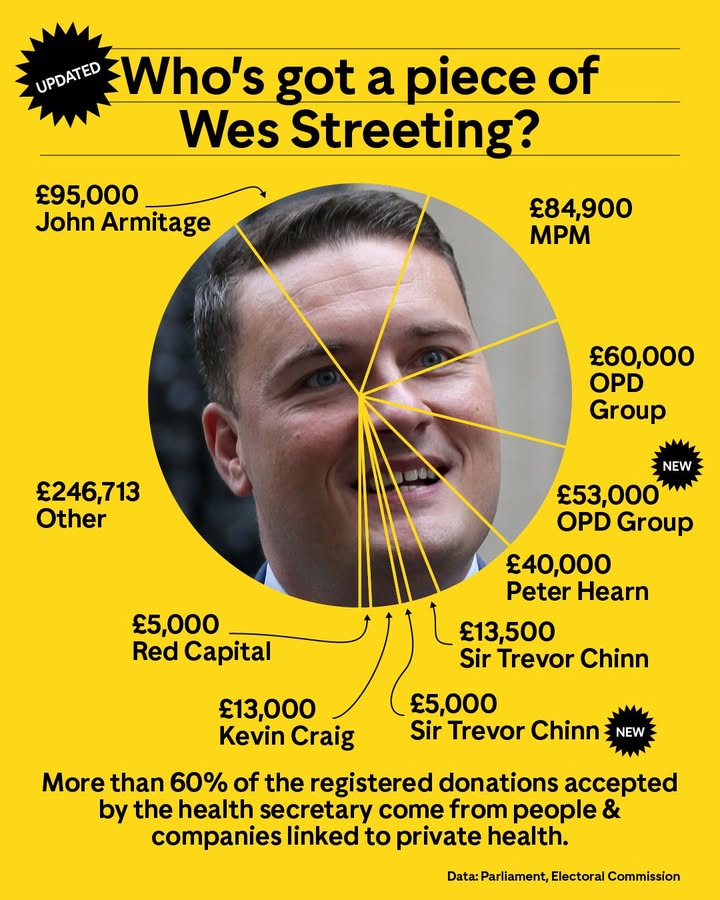
Ban donations to politicians from the US health corporations
Our healthcare costs the government much less per person than the appalling US system. It is more cost-efficient than the European compulsory insurance systems. We need more funding, more hospital beds, more staff, and better buildings. Investment in healthcare builds an economy. Even the World Bank reports that investing in health is key to job creation and growth.
Take the fight for the NHS to the union branches. Make the NHS the talk of the workplace. Let’s not be quiet when people suffer without dignity or privacy on trollies in corridors this winter, not be quiet when babies die from inadequate care in the Maternity service.
There will be a severe political risk this winter if families feel helpless about the problems in the NHS. Our frustrations need a political and community response. Together, we might make the government listen, but the fight goes on even if Starmer continues to have cloth ears. We are fighting for the lives and health of our communities.
We are fighting for lives and dignity. Our area has enormous problems with poverty, and our babies are twice as likely to die around birth as babies in richer areas. Black babies have a greater risk in rich or poor areas, yet other countries do not experience the same problems. This is the outcome of Austerity and neoliberal health policies.
Last winter was grim in all our hospitals, and this year, they face the added burden of funding refusals from NHS England. We saw corridor care for days on end in September, let alone February, long waits in A&E, long waits for beds once “admitted”, and too high bed occupancy for infection prevention. Hospitals are expected to reduce staff as patient needs increase.
The NHS is fundamentally damaged by austerity and privatisation. The government has brought back the worst of New Labour’s privatisation, quacks, and advisers. Billions are being directed to private profit rather than treatment.
The Save Liverpool Women’s Hospital Campaign works with many other NHS campaigns, and we urge people to join us or another similar group local to you.
Contact us, and we will put you in touch or help set up a campaign group in your area. Defend our NHS organises in Wirral and Keep our NHS Public has Merseyside and Cheshire Branches. Most Trades Councils in Cheshire and Merseyside and the NHS camapign groups organise together on NHS issues.
For more information, please see this recent post. Join the campaign to restore, repair, and rebuild the NHS.
Save Liverpool Women’s Hospital.
Make the NHS a core campaign in building a new generation of resistance in the UK. If you are already deeply involved in another core campaign, let’s collaborate on building links. Housing and the environment are key to the nation’s health, as is the right to food. Women’s rights, disability rights and anti-racism work are key to reversing poor outcomes in the NHS. These campaigns should build their links.
If you joined our protest on September 28th in Liverpool (or wished you could have done so), thank you. You are invited to stay in touch to develop ongoing campaigns, to convince others that we can win back the NHS, build understanding and determination, and work together to build a movement so significant that no government can ignore us. Maternity and women’s health have been damaged for many years. We say “Enough is Enough. Restore, Repair and Rebuild the NHS. Repair and rebuild the maternity services and gynaecology care”
We say, as Christabel Pankhurst, one of the suffragettes, said, ” Remember the dignity of your womanhood. Do not appeal, do not beg, do not grovel. Take courage, join hands, stand besides us, fight with us.”
Bread and Roses, the song of women’s struggles, says”As we come marching, marching, we battle, too, for men— For they are women’s children and we mother them again”
Maternity and gynaecology remain a key focus for the Save Liverpool Women’s Hospital Campaign. Please refer to our other posts for more information on this topic.
We can do this!
Working together, experienced and new campaigners, we can gather experiences from the NHS, including those of patients, staff, unions, families, communities, and campaigns.
We each care about the NHS for our own reasons. Some because the NHS has saved their lives or loved ones’ lives, some because of the failures in the NHS, and some because they can see that things could be so much better.
You can and should be allowed a say in how the country organises healthcare. The big corporations that are trying to privatise it don’t want us to have a say, but that’s no reason to be silenced.
We are campaigning for just and effective health economics, as well as the politics of health. This is not the same as practising medicine or providing individual healthcare. That requires qualified professionals, but those professionals are not the arbiters of how a country organises its healthcare. That is a political decision, one to be made, in a democracy, by the people.
Even the World Bank says, “Investing in health is one of the most powerful drivers of economic growth and job creation“.
Modern cities require both public health measures and healthcare for their residents.
Without good public health systems, terrible illnesses rip through the population, as happened in 19th-century London, where even Prince Albert, the husband of Queen Victoria, died of typhoid. Other diseases like Cholera and tuberculosis, smallpox and scarlet fever attacked some of the rich as well as many of the poor. Providing healthcare only for the rich did not protect even the rich. A system of universal healthcare is necessary.
This blog discusses how the UK’s healthcare system is being damaged and how to restore, repair, and rebuild it. It is essential to note that poor housing, polluted air, inadequate food, poorly heated homes with damp and mould, and traffic pollution, as well as a lack of access to green spaces and workplace dangers, including stress and low wages ( the social determinants of health), all contribute to illnesses. We support campaigns for good housing, good food, cleaner air, and decent childcare.
Countries choose from different forms of healthcare. A very few countries leave it to people’s ability to pay and let the rest go hang, much like the UK before the NHS was established. They are mainly in very poor or war-torn countries. Before austerity, the World Bank and other international institutions imposed “structural adjustment” on poorer countries, which damaged healthcare and education. The damage is serious. The UK was severely damaged by Austerity, as other countries had been damaged previously by structural adjustment. This was a political decision of the government. The UK had a choice in this that was not shared by poorer nations
The UK, was the economy hardest hit by Austerity, and it was the poor that were hit, not the rich; “Overall, austerity measures resulted in about 190,000 excess deaths, or a 3% increase in mortality rates, from 2010 to 2019, including many ‘deaths of despair‘.”
“The world is off track to make significant progress towards universal health coverage (Sustainable Development Goals (SDGs) target 3.8) by 2030. Improvements to health services coverage have stagnated since 2015, and the proportion of the population that faced catastrophic levels of out-of-pocket health spending has increased continuously since 2000. This global pattern is consistent across all regions and the majority of countries.”
So political decisions directly affect healthcare.
Health care systems are essential in urban culture, where people live close together and share water sources and drains, as diseases spread too easily.
Some countries (not many) have a fully commercial model of healthcare designed for profit. Because this cannot be easily implemented in an urban environment, the government has to step in and subsidise it for certain groups of people. ( mainly the poor) Some are still left outside the safety net. The USA uses this model of healthcare. It is a cruel and costly model, but highly profitable. It is the system from which many advisers to our Government come; companies involved in the US system are deeply involved in ours. These corporations are exploiting the money that voters think is going to our healthcare. It should not be going to profit.
The US government pays significantly more per person for healthcare than the UK pays per person, and its people don’t all receive coverage; they must also pay for insurance in addition to the government’s contribution. Much of what the US government spends on healthcare does not go to patient care, but rather to insurance companies or healthcare corporations. The NHS model is the most cost-effective, but it generates less profit for large health corporations.
Some countries (like France) have compulsory health insurance with co-pays. Co-pays are where the patient bears some of the treatment costs, and the insurance company covers the rest. This system too has its own problems.It does provide universal coverage; everyone can, in theory, access healthcare, and the nation’s health is good.
Ireland has a complex mix of charges and insurance. People can get some of the fees they have to pay back from the government. Ireland has some excellent outcomes in its health care. “Life expectancy at birth in Ireland was higher than the EU average in 2021, at 82.4 years”
These mixed systems are costly to both individual people and the government.
Even in France’s system, people are employed to administer the insurance and verify it against the hospital charges. Insurance companies and hospitals require numerous administrators. This is money that could be directed to patient care and is, in fact, so directed in the original NHS system.
The UK in 1948 chose the universal public service model on which the NHS is founded. We campaign for a return to the original NHS model. This model is both cost-effective and efficient, and it allowed the system to be recognisedas the best in the world in 2014. Since then, privatisation, along with the introduction of a business model, competition and cuts, has seriously damaged our healthcare.
“Employees, lobbyists, and consultants secure advisory or leadership roles in government bodies and then move back to the private sector. Meanwhile, senior government officials and former ministers take their inside knowledge and contacts to organisations and sectors that do regular business with government.“
The damage to healthcare in the UK during the years of austerity, privatisation, and the ICB system is very well described here by Deborah Harrington from Public Matters. Deborah is a long-term supporter of our campaign.
Please do get involved or continue to be involved. We can win this, but it will necessarily require the involvement of thousands of ordinary people.
There are many different but linked NHS campaigns. Please contact any organisation you might like to work with, and get involved.
Save Liverpool Women’s Hospital; email us at savelwh@outlook.com or reply to this blog post.
Many trade unions work hard on the issues around the NHS, but would welcome activists to do more. Please contact us if you would like to learn more.
Getting more involved can be:
*learning more, sharing your knowledge, or experience,
*talking to people about the NHS
*helping get information out to others,
* organising events, working together to get communities interested,
*getting people interested in the workplace,
*making it clear to politicians that we won’t tolerate unnecessary deaths and suffering any longer.
So, what will the Save Liverpool Women’s Hospital Campaign be doing, opposing or protecting, in the months to come?
• Campaigning to save Liverpool Women’s Hospital and exposing the extent of the national Maternity crisis. For more information, please refer to our other blog posts.
*Campaigning against the Winter Crisis. The winter crisis is going to be grim, as people are already kept on trolleys in corridors for days. We must build the protests about this. Last winter, delays in treatment in unsuitable situations resulted in many lives being needlessly lost.
*Staff shortages and the pressure on hospitals to make redundancies.
Ordinary people must begin to discuss the running of the NHS as if it were indeed their business, and their right. We must remember how we won the NHS and apply those same campaign tactics to win it back.
What would it look like to restore the NHS?
People would be able to get good healthcare more easily.
Migrant charges, which cost so much to implement and bring in less than they cost, would be abolished.
The NHS would once again be a national public service, publicly owned and delivered by people employed in that service. It would be based on cooperation, not competition, between different hospitals.
This model of healthcare provision is much less expensive for the government than the American model. Yes, the American system, where people have to pay huge healthcare premiums, still costs the US government twice as much per person as the NHS costs.
If the NHS were restored, all the privatisation introduced by the 2012 and 2022 Health and Social Care Acts would be reversed. No outsourcing, no privatisation, no use of US models of companies making a profit from our healthcare, no more big US corporations advising on how to run the NHS. No more donations to politicians from private health companies. No more movement of key people between lobbying, working for the private health sector and working in the NHS.
Keep Our NHS Public also wrote that the founding principles included
The NHS asa comprehensive service, universally available, based on clinical need, free at the point of need, and funded through collective contributions.
◼︎that it should be comprehensive – meet the needs of everyone;
◼︎that it should be universal – free to all at the point of delivery to access GP consultations or hospital treatment;
◼︎and that it be based on clinical need, not ability to pay.
We would add that, over the years, building a highly educated and reasonably well-paid workforce was a core part of the NHS. Now, many hospitals do not even pay the living wage, and qualified doctors have no post; nursing and midwifery students are graduating with no jobs to go to (there has been some movement from the government on this, but not a satisfactory resolution).
Campaigns do have an effect. Women got the Vote, we got the NHS, we got equal pay for equal work, we won abortion rights, we stopped the poll tax, and more, all from campaigns and through working together.
It is vital that more people feel confident discussing the NHS with their friends, family, and workmates. It’s very common in the US to discuss the healthcare system; we also need to discuss our system, not just the damage it has sustained. We don’t have to be doctors, nurses, or midwives; we just have to be people.
What would it mean if the NHS were repaired?
Then funding would be improved, and waste that now occurs through privatisation would be redirected into front-line care.
We would begin to recruit enough doctors, nurses, midwives, other health professionals, and ancillary staff to levels that at least match those of other wealthy European countries.
We would have many more hospital beds.
Staff and patients would have more say in the running of the services.
GP services and the entire Primary Care service would be improved.
Public health services would be improved; The Lancet reported that “Public health grant allocations in England have been cut by 24% in real terms per capita between 2015–16 and 2021–22.”
Staff working conditions would be improved, and workload pressures would be eased.
Protest the damage done to the NHS. The NHS belongs to the people. It should be a public service, not used for private profit. The NHS should be well-staffed and well-funded, with all government NHS funds allocated to patient care, staff, and resources.
Protest that the NHS should be fully restored and repaired. No more cuts, redundancies or long waiting lists! Improve Maternity services, restore the GP and dental services.No cuts or hospital closures. We protest the damage done to the NHS and demand complete restoration and improvements in the NHS, for all our mothers, daughters, sisters, friends, lovers and every baby.
The threats to Liverpool Women’s Hospital are part of the general NHS cuts.
Please join us in this protest on 28th September in Liverpool. As the suffragettes said
“Do not appeal, do not beg, do not grovel. Take courage, join hands, stand besides us, fight with us.”
We are protesting on 28th September when the Labour Party comes to Liverpool for its party conference.
Dr Tony O’Sullivan, Co-Chair of Keep Our NHS Public and retired Consultant Paediatrician, said:
“We’re on the brink of disaster. Everyone knows the NHS urgently needs rebuilding—from staff morale and workforce numbers to crumbling buildings and outdated equipment. Everyone, it seems, except the Labour government.”
It is not just Maternity and Gynaecology care that we fight for; we fight for the whole NHS. Excellent life-saving and life-improving care is delivered day in, day out, by the NHS. Some of it is groundbreaking care, and some of it is more routine. NHS staff work hard with great skill and good humour. Pay the staff well. NHS staff should not need food pantries.
Mary Bamber One of Liverpool’s Campaigning women from a century ago.
We say “No! to another winter crisis in our hospitals!” Prepare properly, organise the staff resources and the space now! The Government must provide the funds.
picture credit The Guardian (Nottingham Hospital)
The NHS is ours; it belongs to the people.
The NHSisa legacy from the generation that defeated fascism. A legacy from the women who fought for healthcare for mothers and babies throughout the early 20th Century, often while they also fought for women to have the vote, and it’s a legacy all the women who have fought for our rights since then.
The NHS is a legacy of the trade unions that had set up mini-healthcare systems in mining villages, as well as the unions that demanded universal healthcare. The RMT union has helped publish accounts of how railway workers suffered before the NHS was established. The socialist doctors, some from Liverpool, helped shape early Labour Party policy on health. What would they say about the situation we are facing now with a Labour Government doing such damage?
The NHS is a legacy from those who elected the 1945 Labour Government that set up the NHS, while the country was in staggering debt from World War 2. That Government answered to working-class people, improving their lives, not worsening them.
The NHS is a testament to the countless hours of work that doctors, midwives, nurses, and all NHS workers have dedicated to the service, far exceeding their paid hours in both good times and challenging times.
Yes! We can afford the NHS.
This Government’s excuse is the level of national debt. When the NHS was founded, the UK national debt (from war expenses) was 230% of GDP. Today, it is 95%. It is bad for people and bad for the economy to deprive us of good healthcare.
The NHS was founded to be a universal public service, publicly provided and not for profit. The National Health Service provides healthcare to (most) people in the UK, free at the point of need. It is funded by the Government, like other major services.
The NHS faces major cuts and a long process of privatisation, and the use of NHS funding for private profit. Despite facing understaffing, staff redundancies, underfunding, and crumbling buildings, resources are being diverted to profit private companies, including some very unpleasant ones like Palantir.
No one using the NHS faced bankruptcy or denial of services because of medical bills or lack of medical insurance.
There are many ways to reduce the cost of healthcare, starting with better housing, food, access to heating, insulation, and air quality, all of which contribute to keeping people healthy. However, in 2025, we also need investment in healthcare.
We demand an end to poverty. Maternity Action reported from a survey of women on Maternity leave (with a little baby in the house) that:
One in 10 (10%) of mothers who were using infant formula struggled to afford it. One in four (27%) had cut down on food for the rest of the family in order to buy formula milk.
Nearly three in five (57%) had reduced the number of hours they heated their home.
Nearly two in five (39%) had reduced use of electrical appliances.”
Yet most of these mothers had occupational Maternity pay, not just the very minimum the state provides.
Black Asian and women in the worst off areas re more likely to die in childbirth, or to lose their babies. Liverpool women’s health is set to deteriorate until 2040.
In the 21st Century, the world has made great improvements to Maternity care. In the UK, our maternal and infant mortality rates have worsened while those in other countries have improved.
NHS Maternity is 17th out of 19 comparable countries in infant mortality.
Maternal Mortality is rising, despite fewer births.
The North of England and Black and Asian communities are suffering the worst in infant mortality. In 2022, the UK ranked 19th out of 22 comparable countries, and that has not improved since.
Years of austerity and government cuts have done massive damage to maternity care. Women’s health, life expectancy, and life in good health have all suffered and more so in the UK than in other European countries
What does the NHS do in 2025?
In July 2025, it was reported that each day the NHS provided:
Over 1.3 million people attend a GP appointment.
Outpatient Appointments: Over 304,000 people attend an outpatient appointment.
Emergency Services: Nearly 35,000 people call 999 for an ambulance.
Major A&E: Nearly 46,000 people attend a major A&E department, with about a third of these patients admitted to hospital.
Community Healthcare: Over 288,000 people receive community health care services.
About 1,688 babies are born in England each day,
The NHS is cost-effective and available free at the point of need (to all but migrants, which is cruel and not cost-effective). However, the NHS lags behind other countries’ health systems in the following ways.
A lack of key resources, including the number of doctors per head of population, the number of hospital beds, and the waiting times for treatment.
Important health outcomes, such as certain cancers and life expectancy, are worse in the UK.” By 2023, the UK female mortality rate was 14% higher than the median of peer countries, and the UK male mortality rate was 9% higher.”
Public health issues include housing and food poverty, as well as cutbacks in Public Health Services that work to prevent and control disease. “A report from the UK charity the Health Foundation reveals that public health grant allocations in England have been cut by 24% in real terms per capita between 2015–16 and 2021–22.”
Founded 77 years ago, the NHS fundamentally changed the lives of women, children, and the poor for the better. NHS care outstripped the care previously provided in private hospitals, and the NHS was used by rich and poor, young and old, black, white and brown alike.
Why should we put up with cuts, underfunding, understaffing, and the service being asset-stripped by privatisers?
Every family is affected by the NHS from before conception to the grave. It is with us at our happiest, our most anxious and our saddest times. NHS care affects how long and how well we live.
Restore the NHS as a fully funded universal public service, publicly delivered and government-funded.
Kick out the privatisers and profiteers.
Fund patient care to equal the best in Europe.
Provide the necessary staff. Improve staff pay and conditions. The NHS should be a good place to work, offering good pay, manageable workloads, and time for staff to think.
Fund the repairs and replacement of the necessary buildings to ensure good, timely care.
Don’t fund private healthcare or dubious global corporations that are there to make money and make donations to politicians. Pumping money into the private sector damages patient healthcare.
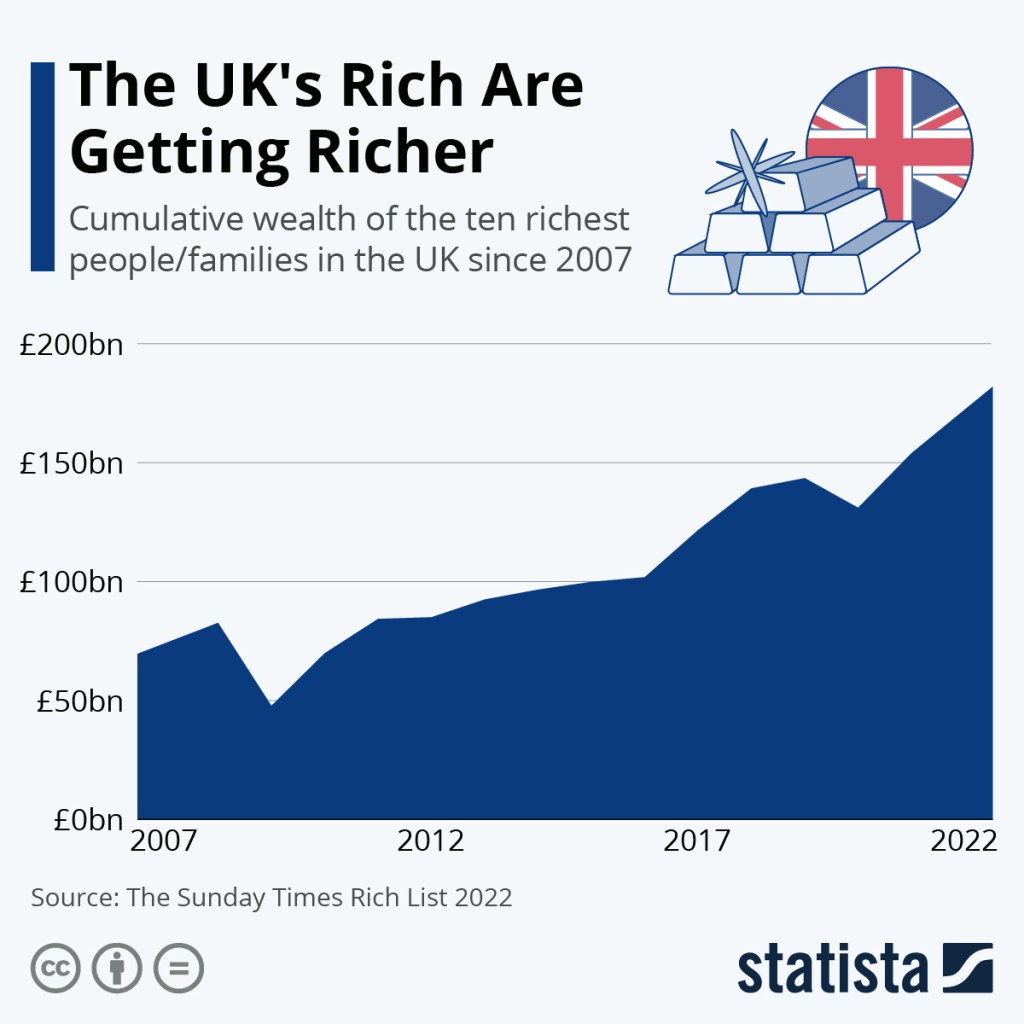
The UK is a very rich country and the rich are getting richer while poverty spreads. It can afford healthcare for all. Indeed, providing universal healthcare is a major investment in the country’s health, wealth and well-being.
The damage done to the NHS over the last few governments is massive. This Government is causing ongoing harm by reintroducing some of the most costly and wasteful (yet profitable for big companies) ideas, such as PFI and Sub Cos.
The (near) universal, free-at-the-point-of-need system in the NHS is an excellent national investment. It gives a good return on the money invested. The cost of collecting fees for health care from migrant workers often exceeds the amount collected.
No solution exists in the US model, regardless of how many government advisers come from that sector. There is a much pushed argument that we can’t afford the NHS, and we should move towards the US health system.US health system corporations are definitely getting claws into our NHS, and they only do that for profit.
In the USA, the Government pays twice as much per person for healthcare. Yet this leaves millions without treatment if they cannot afford the additional insurance. When families can afford health insurance, that insurance can cost as much as their mortgage. Most healthcare plans cover 80% of the cost of care, with the patient paying the rest. What if the 20% is 20% of a very costly treatment like cancer care? One hundred million US citizens owe $220 billion in medical debt. Medical debt can wreck their credit rating and stop them from being able to rent or buy a car on credit.
The USA’s health outcomes are among the worst in the Western world. Maternity and infant mortality are shameful. “The U.S. has the lowest life expectancy at birth, the highest death rates for avoidable or treatable conditions, the highest maternal and infant mortality, and among the highest suicide rates.”
In the UK, we need the Government to;
Reverse privatisation of the NHS in all its many forms
Provide much better funding and staffing in Maternity.
Provide safer, respectful, personalised care for all mothers and babies at every stage of Maternity care.
Bring back quality postnatal care in the hospitals and in the community.
Tackle maternal poverty and food poverty.
End the contract with Palantir, one of the most notorious companies in the USA.
Ban UK politicians from accepting funds from private health corporations or individuals connected to private health or private health insurance.
Fund the NHS to at least good European levels, with all that funding going to the NHS patients, staff, equipment and buildings, not to private companies.
Provide more hospital beds.
“The NHS has a shortage of hospital beds, with occupancy rates consistently exceeding safe levels. The UK has 2.4 beds per 1,000 people; Germany has 7.8 beds per 1000 people. This shortage of beds leads to corridor care”.
Develop a proper workforce planning system, make sure doctors, midwives, nurses and other health professionals have jobs to go to when they qualify. Provide a fully qualified workforce.
Repair our GP service. High-quality healthcare at the GP level should be easily available to all. It is the foundation of good healthcare.
Repair the fabric of our hospitals, clinics and GP surgeries
Bring mental health fully back into the NHS.
Bring dentistry back into the NHS. British Dental Association (BDA) analysis of the data found that nearly 14 million UK adults are unable to access NHS dentistry.
Tackle the waiting lists; don’t fund second-class care in the for-profit sector.
We all need the NHS
From assisted fertility (where needed), to antenatal care, maternity care at birth through postnatal and early years support, through childhood and adolescence, through until old age, the NHS is there to support us. We can all use NHS services, whether in accident and emergency, planned (elective) care, the GP service, mental health services, public health or care in the community. Few are lucky enough still to use NHS dentistry.
If you are younger than 78, you should never have needed to pay for hospital or GP services.
Charges crept in even before austerity for teeth, spectacles, prescriptions and social care. Margaret Thatcher started privatisation in 1982. Her Central Policy Review Staff (CPRS) plan would dismantle the welfare state, scrapping free universal healthcare, forcing people to take out private insurance and charging for education. The CPRS report said, “for the majority the change would represent the abolition of the NHS.” She backtracked when she saw the opposition. She outsourced hospital cleaning, which led to a rise in hospital-acquired infections. Yet even she hesitated to touch the NHS, but later governments have done significant damage.
Social care for our elders was privatised and has become very expensive for individuals and families, unless the NHS pays for it under continuing care. If Social care had been fully nationalised, such payments, either by individuals, families, or the NHS, would not be needed. We would not have been subsidising the profit of hedge funds. Most care homes are private, and many are owned by big business and are very profitable. Much of this profit comes from fees paid by the NHS, local authorities and families. These huge profits are not reflected in the wages paid to staff.
The care provided in our NHS is, many times, excellent, life-preserving, innovative and respectful. NHS staff work hard and often very cheerfully.
Sadly, decades of austerity, privatisation, and mismanagement have caused severe damage to our service.
The 1945 Labour Government founded the NHS. There was hope that it would be improved when Labour won the last election, but we see ongoing damage. Don’t let the damage continue. Save lives—protest for the NHS.
Protest to build a movement like the suffragettes so big the governments are obliged to take action. If enough of us do something about the NHS we can build an unstoppable movement
First posted in June 2024, this post has been updated on August 21st 2025, after Valerie Ann Amos’ “Reflections and Initial Impressions” interim report was published on December 9th 2025 and after the February 2026 Amos interim report.
These two paragraphs, highlighted in yellow, were written after the publication of the December 2025 interim Amos report. Our comments on Amos’ report are at the end of the post.
At the heart of our campaign, and of other such campaigns around the country, is the wish to make Maternity a healthier and happier experience for mothers and babies. We mourn those whose lives have been lost, we send sympathy to those who have been injured, physically, mentally or emotionally, to those caring for injured babies and children and those who have been bereaved. We also care for the staff who have been worn out in trying to make an under-resourced service as safe as it can be.
The people in government, in the top bureaucracy of the NHS and administering trusts, who callously left the service without resources and oversaw the damage as it was being done, must be removed from positions of authority.
Original post
We have been asked to publish this list of the key reports on Maternity issues in the NHS, so they are easy to find. Please let us know of any other reports you know about that we might have missed.
No government can pretend they don’t know about these reports. The campaign for better Maternity care is growing.
These are the many reports on the problems in Maternity care in the NHS. We have provided links to the actual reports and only a brief commentary on some of them.
1. Care Quality Commission 2022/23. There was an update in 2024. It is well worth a read. This is one part of it.”We are concerned that too many women are still not receiving the high-quality Maternity care they deserve. Of the 131 locations we inspected, almost half (47%) were rated as either requires improvement (36%) or inadequate (12%). At 12 locations, ratings for being well-led dropped by 2 ratings levels, and at 11 locations, ratings for being safe dropped by 2 levels.”
The CQC are also quoted in the BMJ report as saying, under the heading Acceptance of Shortfalls:
“On the basis of these findings the CQC has set out recommendations for NHS trusts and integrated careboards, including ensuring that they are collecting the right demographic data and then using such data when reviewing and acting on patient safety incidents. The regulator has also called on NHSEngland to work with the Nursing and Midwifery Council and the Royal College of Obstetricians and Gynaecologists to “establish a minimum national standard for midwives delivering high dependency Maternity care.” It urged the Department of Health and Social Care to provide additional, ringfenced funding for Maternity services. Nicola Wise, CQC director of secondary and specialistcare, said, “Sadly, our latest maternity inspection programme has further evidenced the need for urgent action, with continued problems indicating that the failings uncovered in recent high profile investigations are not isolated to just a handful of individual trusts.” and “We cannot allow an acceptance of shortfalls thatare not tolerated in other services. Collectively, we must do more as a healthcare system. This starts with a robust focus on safety to ensure that poor care and preventable harm do not become normalised and that staff are supported to deliver the high-quality care they want to provide for mothers and babies, today and in the future.”
2. Donna Ockendon Donna Ockendon produced the Shrewsury report and has gone on to do more. This interview with Donna Ockendon is useful too, especially the last section. This interview is also informative. Donna Ockendon is working on a report on a long review of Nottingham’s Maternity services. This video from Donna Ockendon explains some of it.
11. There is a summary of many reports on Maternity safety from the House of Commons Library here.
12. There was a worrying report from the CQC about Maternity services in Leeds General Hospital in 2024. There was also concern reported about the neonatal unit. A later 2025 report indicates some improvement, but still requires an improvement report.
13. The government has announced on June 23rd 2025, a rapid enquiry into Maternity Safety following meetings with bereaved parents. This is the announcement.
14. The Health Services Safety Investigations Body produced a summary in advance of the government’s proposed rapid enquiry. It can be found here.
15. Then there was the announcement of the name of the leader of the enquiry.
16 Meanwhile, the government will investigate ten Maternity services that are causing concern. Then there will be a system-wide investigation. This is the relevant document. The different responsibilities of the task force and the investigation have yet to be clarified. The bereaved parents, who met Wes Streeting, wanted an investigation by someone outside the NHS, which is why Baroness Amos was appointed as someone independent of the NHS. Baroness Amos is a Labour member of the House of Lords and has had many responsibilities, including being the first black woman cabinet member. Baroness Amos delivered a speech on women’s health, with a particular focus on black women’s health, in the House of Lords on International Women’s Day 2024.
17. Thisfrom the BBC about the recent coroner’s inquest into Ida Lock’s death sums up many of the reports.
18. Though not directly related to Maternity, this report on Women’s Health, published in Parliament in March 2025, is also important.
19. The particular risk to black mothers was reported in 2023 in Parliament. There are campaign groups on this issue, including https://themotherhoodgroup.org/, and FiveXMore have produced a detailed reportand recommendations, well worth a read.
20. A report was published in The Lancet in May 2024 by Nicola Vousden, nicola.vousden@npeu.ox.ac.uk,∙ Kathryn Bunch, ∙ Sara Kenyon ∙ Jennifer J. Kurinczuk, ∙ Marian Knight, on the particular risk to black women reported this; “There were 801 maternal deaths in the UK between 2009 and 2019 (White: 70%, Asian: 13%, Black: 12%, Chinese/Other: 3%, Mixed: 2%). Using the routine data comparator (n = 3,519,931 maternities) to adjust for demographics, including social deprivation, women of Black ethnicity remained at significantly increased risk of maternal death compared with women of white ethnicity ( our emphasis )(adjusted OR 2.43 (95% Confidence Interval 1.92–3.08)). The risk was greatest in women of Caribbean ethnicity (aOR 3.55 (2.30–5.48)). Among women of White ethnicity, risk of mortality increased as deprivation increased, but women of Black ethnicity had greater risk irrespective of deprivation. Using the UKOSS control comparator (n = 2210), after multiple adjustments including smoking, body mass index, and comorbidities, women of Black and Asian ethnicity remained at increased risk (aOR 3.13 (2.21–4.43) and 1.57 (1.16–2.12) respective 22. The Royal College of Gynaecology produced a position statement on poverty and women’s Health, including the impact on Maternity.“Poverty (lacking financial resources to meet needs) and deprivation (lacking many resources,including those that shape our health), can have a significant health impact across women’s lives. This includes cutting lives short. Across the UK, women living in the most deprived areas have a life expectancy many years shorter than their least deprived counterparts. In England, the disparity in female life expectancy between the most and least deprived areas is eight years, with those from the most deprived areas also living 20 years fewer in good general health. Similar disparities are found in Scotland, Wales and Northern Ireland.
This report on the buildings used for Maternity and Neonatal care is shocking. In some places, the birthing rooms are too small to accommodate emergency equipment. The very fabric of the service is substandard. Again, this is a government report, so the politicians know what’s going on and are letting it happen.
22.The Amos interim report, December 9th 2025. It is essential to point out that while some of these issues may well apply to Liverpool Women’s Hospital, these criticisms are not directed at it. There is good practice at Liverpool Women’s Hospital on some of the issues mentioned below. Liverpool Women’s Hospital is not one of the hospitals being studied in this report. But we fight for all Maternity services, not just Liverpool Women’s Hospital.
Valerie Ann Amos’ interim report includes these statements.
“..nothing prepared me for the scale of unacceptable care that women and families have received, and continue to receive, the tragic consequences for their babies, and the impact on their mental, physical, and emotional well-being.
While the issues I have heard about through this engagement have been extremely varied, there are a set of issues which I have heard about consistently. These include:
a lack of communication and support from clinical teams and organisations
women not being listened to or given the right information to make informed choices at critical moments of their care as risk profiles change
women’s knowledge of their own bodies and important information essential to clinical decision making about their care, such as reduced fetal movement, sometimes being disregarded
fathers and non-birthing partners feeling unsupported
the desire for a more holistic approach to care across a woman’s maternity and postnatal journey, with maternity and neonatal teams working together to maximise good outcomes for women, their babies and families
the impact of discrimination against women of colour, working-class women, women with mental health challenges and younger parents, leading to poorer outcomes
a lack of empathy, care or apology, both as part of clinical care and after things have gone wrong, with women feeling blamed and guilty; a lack of recognition from staff when care is not delivered to the correct standards
lack of family engagement in reviews of care and feedback of review reports
an overly legalistic, adversarial approach when concerns or complaints are raised
the failure of regulatory bodies to protect vulnerable women and families and the perception of health professionals and organisations ‘marking their own homework’
failure to address poor behaviour, including the use of inappropriate language when communicating with women, families and non-birthing partners
the length of time autopsy reports take to be produced, delaying families from being able to fully grieve for their children
poor standards of basic care, such as lack of cleanliness, women and non-birthing partners not receiving meals, women not being helped to use the bathroom, and cathetershttps://www.england.nhs.uk/long-read/the-maternal-care-bundle/ not being checked or emptied
women and families finding it difficult to access their medical notes (and notes being redacted or observations filled in at a later date)
birth plans not being read or followed, leading to women not being cared for in the way they wanted or had agreed, as well as having to repeat their wishes multiple times
women and families being placed in inappropriate spaces after loss or harm, for example, being put on wards with newborns after they have experienced a loss
the impact of different philosophies around birth and pregnancy on women’s experience and ability to make informed choices
having to work with multiple contacts when a baby dies, with issues arising from information not being shared sufficiently between different services
the lack of recognition of, and support for, the long-term impact that these negative and traumatic experiences of services can have on families, for example: family breakdown; long-term impacts on the mental health of women and families; support for raising children with lifelong disabilities; bereavement care; participation in reviews or investigations; joint planning of complex care; and the need for neonatal unit accommodation and transition care I have also heard from some families about the high-quality, compassionate care they have received.
The staffing levels and the spaces in which the care is delivered are not mentioned. This is important; if ignored, problems will persist. Stephanie, one of our retired midwife campaigners, said, “You get one chance to deliver a baby safely. There are no reruns or repeats. The accoucher must get it right every time. To do so, the midwife must be supported by her colleagues, midwifery management and work within a fully safe environment. Alas, with the fragmentation of our NHS, top down draconian management, our mothers, their babies and our midwives are give short shift and they become the victims of often tragic circumstances. There is a woeful shortage of skilled midwives. Anyone can deliver a baby but it takes a skilled midwife to do so day in day out safely and with professional accountability.“
We are also concerned about the speed with which some of the hospital visits in the enquiry are planned. The report says
“For the remainder of December 2025 and in January 2026, the programme of site visits to hospital Trusts will continue. The Trusts to be visited are:
• Blackpool Teaching Hospitals Foundation NHS Trust
• University Hospitals of Leicester NHS Trust
• University Hospitals Sussex NHS Foundation Trust
• Sandwell and West Birmingham Hospitals NHS Trust
• University Hospitals of Morecambe Bay NHS Foundation Trust“
This doesn’t seem like an adequate time to gather anything except prepared comments from management. It is more than one hospital a week, and key reports will be published based on these snapshots. What else will be considered?The report does say” We have spoken with frontline staff, who have been open and frank about the pressures they are under, their experiences working in maternity and neonatal services and about the areas that require improvement”
And what will happen to managers who spill the beans about inadequate staffing, inadequate buildings, and the inadequacy of the Maternity tariff? Or criticism of Birthrate+, the tool used to determine staffing levels? Will they have whistleblower protection?
The visits are not the only work still to be done for this report. The author says
“I also want to make sure that we are hearing views from staff across the country and amfinalising plans for how we will collect this evidence.
The enquiry will also meet a range of people from the NHS hierarchy. Will they also meet the unions and the campaigns?
Also
23. The Maternal Care Bundle, 16th January 2026, indicates clear governmental knowledge of the scale of the problem.
The latest MBRRACE-UK data (2021 to 2023) suggests that maternal mortality has increased by 21% since 2009 to 2011, or 7% excluding deaths relating to COVID-19 infection. In addition to coronavirus, demographic trends such as rising maternal age, obesity and prevalence of pre-existing medical conditions are making maternal care more complex. Stark disparities in outcomes persist. In 2021 to 2023, Black women died at more than twice the rate of white women, and women living in the most deprived areas died at almost twice the rate of those in the least deprived areas. Disparities are also evident in maternal morbidity; among women giving birth in England between 2016 and 2021, 1.6% experienced a severe morbidity with odds up to 89% higher for Black women and 20% higher for women living in the most deprived areas (Geddes-Barton et al 2024). MBRRACE-UK assessors felt that improvements in care could have made a difference for 45% of the women who died between 2021 and 2023. While significant action has been taken in recent years at trust, regional and national level, this data illustrates the urgent need for more consistent, high-quality and equitable care across England.
24. February 2026 Independent Investigation into Maternity and Neonatal Services in England – Interim Report by Valerie Amos
On Thursday, 24 July 2025, campaigners to Save Liverpool Women’s Hospital attended the meeting of the Cheshire and Merseyside ICB and asked a formal question, in writing, of the ICB about when the timeline for the future of the Women’s Hospital would be published:
“There is mention in the papers that a timeline for the next stage of the plans for Liverpool Women’s Hospital has been submitted to the chair of the ICB. When will the public be informed of this timeline?”
We want Liverpool Women’s Hospital to remain at Crown Street, with improved funding, staffing, equipment, and cooperation with other hospitals, for the benefit of all our mothers, sisters, daughters, friends, and lovers, and every baby.
This is what the “Women’s Hospital Services in Liverpool” published. Their words are in italics. Our comments are in plain text and sometimes highlighted in yellow.
“The NHS is looking at hospital gynaecology and maternity services in Liverpool.
Most of these services happen at Liverpool Women’s Hospital, on Crown Street in Toxteth, which means they are separate from other hospital services, and this can sometimes create issues and delays with care.
The NHS is committed to finding a long-term solution that will improve the quality and safety of hospital gynaecology and maternity services, giving patients the best experience, wherever they are being treated.
Current timeline
What’s happened so far during 2025
March: Women’s Services Committee received a report into the autumn 2024 public engagement and approved the options process. The Board of NHS Cheshire and Merseyside also received the public engagement report, and it was published on the programme website.
(Our comment: Campaigners attended every meeting of this engagement, and not one of the meetings supported the position put by the ICB team. We produced a detailed rebuttal of their case, which we submitted to them. We are told they have considered the points we made, but no such consideration appears here. Their report continues…
What’s underway now and coming up (future dates still provisional and could change).
May to September 2025 – options process: Local doctors, nurses and midwives, those with lived experience of gynaecology and maternity services (members of our Lived Experience Panel), and other partners, have been coming together in workshops to develop potential options for how services could look in the future. Alongside this, work is taking place to understand what each potential option would mean for estates (buildings), finance and workforce (staffing).
None of the options discussed in the paragraph above are described or explained. These options are clearly getting out into the community, creating uncertainty and confusion. Why is that? Surely the ICB papers are the formal record of its business, and should include such vital details. The report continues…
July to October 2025: Development of a draft business case for the future of hospital gynaecology and maternity services in Liverpool, including potential options, begins.
October 2025: The Women’s Services Committee to review draft business case.
October to November 2025: Discussions with partners, including local NHS trust boards and local authorities, about the draft business case. At this point we will also start planning for an external review of the draft business case by clinicians from a different part of the country.
November 2025: Draft business case presented to private meeting of Board of NHS Cheshire and Merseyside.
By the end of 2025, we will be in a position to understand the next steps for the programme – it’s likely that we’ll be able to give an update about this in early 2026. It’s important to stress that no final decisions about what services might look like in the future will have been made at this point, and if the decision was to take forward a business case containing potential options, we would then continue with the NHS England assurance process, external clinical review, and planning the public and stakeholder involvement required.
This long-winded and expensive project, which has cost many tens of thousands of pounds, continues while the hospital and the ICB are desperately short of funds. It leaves patients and the entire community in uncertainty. The real work of improving services at Crown Street is underway at the hospital. In another report to the same ICB meeting, the Women’s Hospital Services in Liverpool report confirmed that ; Risk 6 – onsite quality and safety – the LWH team has made great progress over the last twelve months, and the score could be brought down, this will be discussed at Programme Board on 21 May 2025.
While the ICB’s process is happening, there is a Maternity crisis in England with report after reportdescribing the grief and suffering involved. The NHS as a whole is underfunded, understaffed, and damaged by privatisation, and if this ICB meeting is anything to go by, it is getting even worse for patients and staff. We will report more of what happened at the ICB in a future post. Much of the rest of the ICB meeting was about further cuts and Cost Improvement Programmes.
The report of the Women’s Hospital services in Liverpool to the ICB in July confirmed that;
Risk 7 – a new risk has been added regarding staff reductions in the NHS and the potential impact on the programme. The programme budget has been agreed, however as the staff reductions are made throughout the year, there could be implications for the programme.
Liverpool Women’s Hospital is the largest Maternity hospital in the country. It is the Maternal Medicine Centre for the wider area, where other Maternity hospitals go for advice on complex cases. It should be well-funded, well-staffed, well-equipped, and well-supported. At the heart of the problems of Liverpool Women’s Hospital are;
1. The underfunding of Maternity across the country, an underfunding that has cost so many lives.
2. Utterly stupid policies, including the 2012 Act, meant hospitals were supposed to compete rather than cooperate with each other. This requirement has technically been removed, but the business model remains. Cooperation between the Women’s and other hospitals was difficult and expensive.
There should be NO staff reductions in this situation, especially as these reports from the same ICB (pages 146-150) from the Women’s Hospital Services in Liverpool Committee confirmed the real poverty many of us who use the hospital currently endure.
“Almost two-thirds of maternity bookers lived in the 20% most deprived areas in the country. Our partner hospitals in Liverpool University Hospitals Trust ranked in 2020 as having the most deprived catchment population of any acute trust (NICE and health inequalities, 2025). “Based on recorded ethnicity and deprivation alone, 70% of maternity bookers 75% of emergency gynaecology admissions50% of elective gynaecology admissions have at least 1 risk factor for healthcare inequalities…..64% of maternity bookers 71% of emergency gynaecology admissions 52% of elective gynaecology admissions live in the 20% most deprived areas in the country.”(Appendix to Women’s Hospital Services in Liverpool Committee report). These papers also confirmed the significant gap between the lived experiences of decision-makers and the women using the hospital.
“There is a significant difference between demographics and experiences common among senior decision-makers and common among our patients. Designing services for the white and well-off would focus on about 10% of our maternity and emergency gynaecology patients.” (Appendix to Women’s Hospital Services in Liverpool Committee report).
The NHS has a duty of candour. Where is this duty here? The NHS belongs to the people. Why are such contentious discussions not described to the public, if the NHS belongs to us?
More than 81,000 people have signed our petition, to keep Liverpool Women’s Hospital at Crown Street, signed either on paper or online, and thousands have taken part in our protests. We have produced a detailed and comprehensive rebuttal of the ICB’s engagement process.
Keep our campaign growing to Save Liverpool Women’s Hospital. Sign our petition. Talk to your friends, family and workmates. Join our protest on September 28th.
This is part of the neglect of the NHS and of women’s health services. We demand that the NHS be Restored and Repaired!
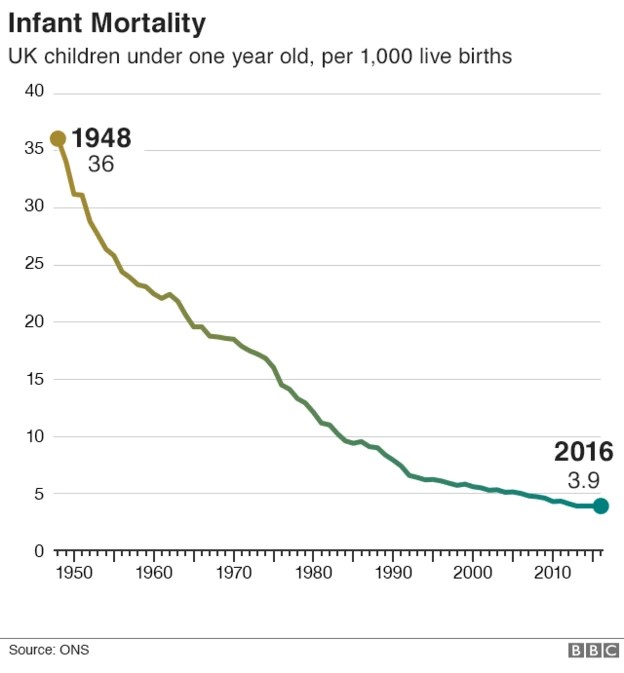
It is seventy-seven years since the NHS was founded. It was a gift to the generations that followed them from those who fought all-out war and defeated fascism in World War 2. It made a dramatic difference to the lives of babies and mothers.
Before the NHS, if you did not have the money, you did not get healthcare. The number of babies that died at birth was horrific. In the 1930s, more women died in childbirth than men died working in the dangerous mines.
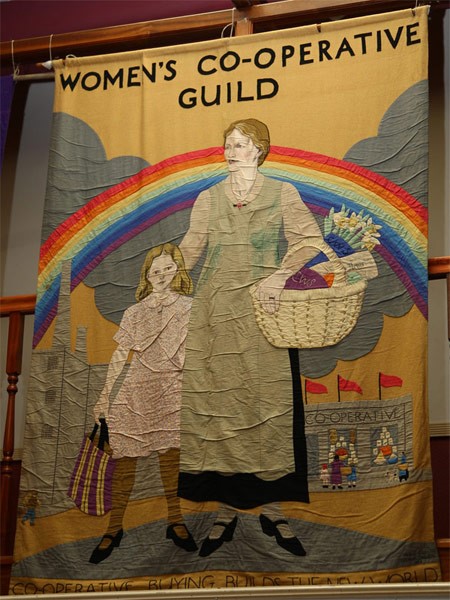
There were multiple campaigns for a universal health system since the early 20th Century from working-class women’s groups, notably the Cooperative Women’s Guild, and from the trade unions, especially the National Union of Miners, and from socialist doctors. One of these socialist doctors, Dr Benjamin Moorewas from Liverpool. He started his campaign in 1910, so thirty long years before the NHS was established. Let’s learn from history and demand a return to the original model of the NHS.
Join our campaigns so you can see better healthcare in your life time and leave such just a legacy for your grandchildren and great-grandchildren. We need a people powered campaign to Restore and Repair the NHS.
Ordinary women led the fight for the NHS. Fight like your great Grandmothers to get better health care.
The NHS is badly damaged at present, and we take little comfort from the government’s liking for giving NHS money to the private providers, nor from the Ten-year Plan announced in early July 2025 https://www.england.nhs.uk/long-term-plan/
We will print a detailed review of this plan shortly.
We are especially disappointed by how little is said about the state of maternity care in this report. We and other maternity and women’s health campaigns submitted reports to this plan, but we see nothing from it except the promise of yet another report. We need action now on birth trauma, the maternity tariff, staffing levels, recruitment and retention of staff, peace and respect in the whole process of fertility, pregnancy, giving birth and postnatal care. We need action on the neglect of Gynaecology treatment and on women’s lifelong health and healthcare,
Governments since Thatcher have moved against the founding NHS model of universal health care in favour of allowing companies to use it for profit; yet the American system which they base their case on, is plain wrong, cruel, and widely hated.
Let’s ensure that people in the UK now and those yet to come have good and timely healthcare, free at the point of need, as a public service, funded by the state. It should be a national organisation available to all humans, young and old, black, white and brown, rich and poor alike. It should be designed for human good, not profit. There should be well-qualified staff with good education and training, with bursaries and good salaries. The hospitals and community health services should work together and not be in competition. The service should be reasonably close to home with good transport links. Privatisation should become a thing of the past, as it is a waste of public resources. Report after reportdescribes the damage done by outsourcing and privatisation.
The NHS system of health care is cost efficient, and effective, far cheaper for the government than the US system despite the health insurance people pay, and gives far better outcomes, health, and life expectancy. We live longer than people in the US and in less fear of getting ill. US maternal mortality and infant mortality is far higher than that of other rich nations.
Let’s fight to restore and repair the NHS so the generations that follow us are also free from fear. Bevan’s book “In Place of Fear” wrote of the fear ordinary families had of getting ill, of their children or family members falling ill, before health care was a right, when it was a commodity they could not afford and often did without, in pain and fear. Memories of life before the NHS are fading as the generation that created the NHS has passed.
The NHS improved the health and wealth of the nation and even conservative governments had to pretend to be in favour of the NHS
The founding of the NHS was bitterly opposed by the Conservatives but welcomed by ordinary people and many GPs.
For seventy-seven years, the people of Britain have had the right to healthcare free at the point of need. If you are younger than 77 years old you need never have paid for healthcare, except through your normal contributions to the country. There are now sadly a long list of charges you might now face for dentisty, for prescriptions, for earwax removal, fertilty treatment and more but still not for hugely expensive life saving operations or chemo. Battered and damaged, the NHS is still alive and kicking, and worth us demanding its restoration and repair.
People in the UK can still go to the doctors or to the hospital without a credit card or health insurance. No one in the UK needs to go bankrupt from medical bills. life saving and life improving work is delivered day by day.
That’s not the way it works in the USA; the model that governments refer to when they want to make changes to the NHS.The model that has trained the advisers the government appoints and the model liked by many who have made donations to Government ministers.
For sixty of those years, the NHS was the best health service in the world. However, we have had to fight to defend it again and again. That popular defence is needed now more than ever.
Americans camapigning for full health care
Real damage has been done to the NHS since the time of Margaret Thatcher, by her and and subsequent Governments. Although Blair put money into the NHS, he also laid the groundwork for many forms of privatisation. This article gives a timeline of privatisation in our NHS.
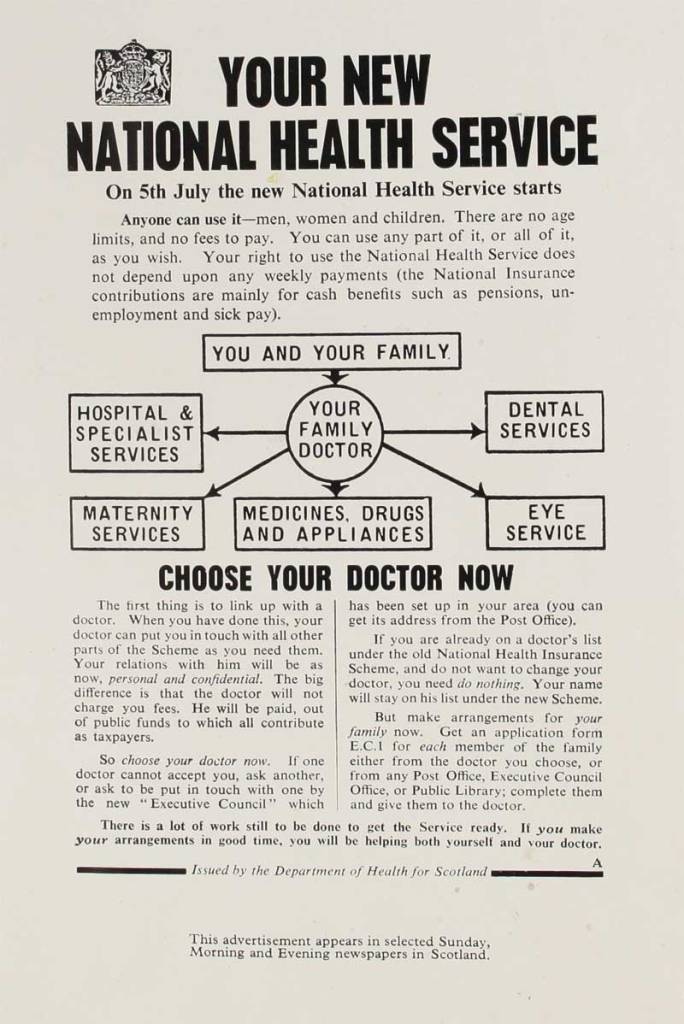
5th July 1948, The National Health Service NHS was founded. It was designed to provide healthcare free at the point of need for everyone in Britain. It was to be a national, publicly funded, publicly delivered, comprehensive, not-for-profit health service, with fully qualified staff. This project was led by the Left-Wing Labour MP and Minister for Labour, Nye Bevan, a former miner.
The NHS Model was the most cost-effective, efficient, and equitable system, with the bulk of the money provided by the government going directly to patients, staff, and buildings. In the US system, the government pays twice as much per person as in Britain, and then patients have to pay large insurance premiums and copays.
The NHS has been badly damaged by years of privatisation and underfunding, from the early days of the NHS. On April 23rd 1951 Bevan resigned when the first charges in the NHS, for prescriptions, were introduced to pay for armaments.
It is likely that governments thought that privatising, disorganising, cutting, outsourcing understaffing and underfunding the NHS would finish it off, that it would fall apart much more than it has done. What stood in their way was the huge and relentless efforts made by the staff to keep the service going, sometimes at the cost of their own health and wealth.We thank the NHS staff .
The cost of the corporate profit model of healthcare is huge, but the damage is not just to people’s money, but also to access to healthcare and to the quality of care. The financial cost to the people of the USA of this privatised for-profit model of healthcare is estimated at $2 trillion per year. In 2023 25.3million people in the USA had no health insurance and are liable for the full cost of their treatment which can lead to bankruptcy. Sixty percent of all bankruptcy is caused by medical bills and Trumps Big Beautiful Bill which just went through the senate is likely to increase the numbers without health insurance and funding for hospitals.
Our campaign to Save Liverpool Hospital is one of many across the country, and we work together. We have won more than 81,000 signatures between our on line and on paper petitions, and gained much public support. Please join in.
Use the links if you wish, but they are not essential to understanding the information.
The campaign wagon that we use when we can collect enough donations.
NHS University Hospitals of Liverpool Group Board meeting.
As members of the public, we have attended the ICB and the Liverpool Women’s Hospital Board meetings for some years and attended the NHS University Hospitals of Liverpool Group Board meeting on June 5th, 2025.
We heard that because the ICB was refused the funding it requested, all Cheshire and Merseyside Hospitals and many other services must change their financial plans for the worse. However, the Trusts are not allowed to reduce their planned services! This must increase pressure on the frontline NHS workforce. Staffing is a large part of all NHS spending and is crucial to patient care.
Note: “Cost Improvement Plans” are cuts. Yes, a large organisation like the NHS must be on the watch for potential savings, but the system is used to enforce cuts.
The ICB reported that “On April 30th 2025 the ICB submitted a compliant plan ( which has resulted in both the ICB and every Cheshire and Merseyside Trust provider taking on additional cost improvement requirements (resulting in an aggregate deficit across the 16 NHS providers of c£228m offset by a surplus for the ICB of £50m). This compliant plan will enable us to spend our allocation, plus the additional £178m of deficit support funding (equivalent of 2.2% of our allocation) during the2025/26 financial period. Whilst agreeing a plan was essential to securing the deficit support and cash to underpin this, our attention must turn now to the effective delivery of the plan and effectively mitigating the risks“.
Like Oliver in the workhouse, the ICB asked for morePicture credit
See our commentary on the May 2025 ICB board here.
We have always opposed the ICB system imposed by the 2022 Health and Social Care Act. Streeting is giving us more of the same.
We have observed how trusts negotiate their funding with the ICB. They agree on a plan for services, treatments, and the required money. It is a complex operation with oversight from outside bodies. The ICB takes all the plans for all the services in the area to NHS England and agrees on funding levels. Negotiations continue during the year for next year’s funding. The NHSE rewards trusts that do well in certain areas and has just announced some capital funding for buildings and extra services, including mental health in the acute hospitals. This, though, we are told, is not additional money. This carrot-and-stick funding is inappropriate and wasteful; it just lets a few positive headlines help some MPs.
The ICBs ( separate and distinct from the Hospitals and provider services) facesignificant cuts in their functions and funding as Wes Streeting implements his peculiar plans for the NHS.
The Health Service Journal reports that his year, “Integrated care boards and trusts are collectively aiming to make efficiency savings of 7.1 per cent or £11bn.”
These cuts are imposed while the winter crisis in our hospitals lives on through the summer in some places and is unlikely to improve next winter. At the same time, we have unemployed GPs, people needing GP care, and more than six million people waiting for treatment.
Women’s health sees some of the longest waiting lists, and our Maternity outcomes urgently need to be improved. Women hold up half the sky and make up nearly 80% of the NHS workforce. They are more likely to think of the NHS when voting. Yet our healthcare is disrespected in so many ways. The country has a Maternity crisis, and mental health care is severely damaged.Social care is a disgrace.
Liverpool Women’s Hospital is now part of the NHS University Hospitals of Liverpool Group, which comprises The Royal, Aintree, Broadgreen, and Liverpool Women’s Hospital. Other Liverpool Hospitals will also join the Group soon. “Liverpool Heart and Chest will join by September this year, the Walton Centre by December, and the Clatterbridge Cancer Centre by March 2026.”
(No, you didn’t miss the public consultation about the creation of this Group because there was none.)
Liverpool Women’s Hospital is still technically a separate Trust; however, the final say now rests with this group board, none of whom, as far as we can tell, have obstetric or midwifery expertise.
“Although LUHFT and LWH will remain in operation as statutory entities, in all other aspects, they will delegate authority to NHS University Hospitals of Liverpool Group (UHLG)”.
Hospitals receive funding via the ICB. They also agree on their planned treatments and urgent and emergency care Plans with the ICB. The Trusts are paid for what they plan to deliver.
The Trusts and the ICB had drawn up these plans in detail. NHSE had appointed outside bodies, like Price Waterhouse Coopers, to work with the Liverpool boards and the ICB to oversee their finances and to reduce spending. It was just such a worked-out package that NHSE declined. Further, NHSE would withdraw previous deficit funding of over £176m to Cheshire and Merseyside if the books were not balanced. Each Trust was given far less money than they expected.
The CEO of the Liverpool Group explained that, having received less funding, they had to decide which services to cut. But, they were then told they still had to meet the original service targets with less money.
So, Liverpool Women’s Hospital is facing more financial problems. It is a small hospital whose funding is determined by the Maternity tariff, and the Maternity tariff( funding) is inadequate across the country.
These national cuts are a policy decision distinct from previous years. They come after years of Austerity, privatisation, and underfunding in the NHS. Sadly, this Government’s policies are little different from the last.
Campaigns do make a difference. If you fight, you might just win.The more people involved, the more likely we are to win. So, we have to campaign harder and draw more people into the campaigns to Restore and Repair the NHS.
The NHS came from ordinary people, unions, women’s organisations and community groups. That is to whom we must turn again. Please join the campaigns to restore and repair the NHS. Contact us for details on how you can help.
There may well be some waste and overspending in the NHS. These cuts happen while more than six million people are waiting for treatment. Some treatments, like those for endometriosis and young people’s mental health, need to improve. We need democracy and community oversight in the NHS.
When our campaigners go to meetings and read their papers, we still have limited sight of what’s going on and only retired people really have the time to attend these meetings.
On June 5th, we could not even hear crucial sections of the meeting where significant changes in the funding and delivery of services were being discussed. We were “told off “for asking them to speak up in what is supposed to be “a meeting held in public.” They have promised to use microphones at the next meeting. There is no effective democratic scrutiny of the NHS.
This new board format shows less detail of Liverpool Women’s Hospital matters. We do not, for example, see the staffing fill rates for different services as an issue that matters very much to women giving birth. From the reports that we did see, we learned that Liverpool Women’s Hospital has a significant waiting list for Gynaecology treatment:
“Gynaecology remains a challenged speciality nationally in terms of long waits and capacityconstraints. At LWH, referrals into the Gynaecology suspected cancer pathway havesignificantly increased over the last 3 years, increasing from 3,500 per year in 2021/22 to 6,000 per year in 2024/25 – a 71% increase. Demand has been exacerbated by changes in the Post Menopausal Bleeding pathway as well as significant long waits for General Gynaecology services. LWH is also the Tertiary provider for Gynaecological Cancer across Cheshire & Merseyside.” Page 239 in the Board papers
The hospital is opening three new “ambulatory” (daytime) treatment rooms. However, increased demand has already shown a need for still more capacity and money to fund that capacity. We were told that close work with other cancer teams across the Group and support from across Cheshire and Merseyside are helping to develop an effective plan to drive down this waiting list.
Gynaecology has one of the longest waiting lists across the country.
In March 2025, Endometriosis UK wrote New data shows the non-cancer gynaecology lists continuing to stand at over 580,000 women in England alone, with women waiting months and even years with serious, progressive conditions, including endometriosis.
In December 2024, The Guardian wrotethat waiting lists for gynaecology appointments across the UK had more than doubled since February 2020. Records show around three-quarters of a million (755,046) women’s health appointments are waiting to happen – up from 360,400 just before the pandemic..
The NHS should be a nationwide, publicly delivered, well-funded and well-staffed service. Our campaign always called for cooperation between hospitals and rejected the Conservative ideas of competition between hospitals and bringing the market economy into the NHS.
Unsurprisingly, pressure is being put on the workforce to work harder. All kinds of stunts are coming in, like outsourcing, insourcing (not the same as bringing services back in-house), changing how bank nurses are paid, not filling vacancies and more privatisation. Privatisation is not more cost-effective, nor does it deliver better patient outcomes. Services, too, will be cut.
It is unacceptable that the Government is imposing such a scale of cuts while we wait for treatment.
We learned little of the plans currently being drawn up for the future of “Women’s Hospital Services in Liverpool”. We questioned whether staff at LWH had been told that one option was a new build on the Royal site. It seems it was mentioned at a staff briefing, but only as a reference to the options years ago. The ICB had categorically ruled out a new build for Liverpool Women’s Hospital on the old Royal site, and the site has been agreed upon as a new building for the university. The Echo reported on June 5th about more details for the site of the old Royal, including an improved entrance to the Royal Hospital. There is no mention of a rebuild for Liverpool Women’s Hospital, although plans can change until construction starts.
We want the Liverpool Women’s Hospital to be properly funded and staffed and to remain on the Crown Street site in cooperation with other hospitals.
“Save the Liverpool Women’s Hospital. No closure. No privatisation. No cuts. No merger. Reorganise the funding structures, not the hospital. Our babies and mothers, our sick women deserve the very best.”
Why is this important?
All the maternity and women’s health provision of Liverpool was pulled into this one site. It’s a much loved hospital. It provides crucial specialised care and the daily joy of new babies. #one born. The driving force for closure is a clumsy funding structure not the needs of women and babies. The alternative of wards in the new Royal is not an equivalent.
This is a modern hospital on a good site. Our taxes built it for our babies and for our women.“
We campaign to save Liverpool Women’s Hospital, to Restore, Repair the NHS, and to make the NHS a great place to work. Please help. Combining our paper and online petitions, we have 81,470 signatures. Please help us get even more. Our work includes petitions, leaflets, stalls, rallies, working with other Maternity campaigns and with community groups, unions, Keep Our NHS Public, and other NHS campaign groups, our Facebook page, and this blog aims to provide information and help campaign organisation.
Proposals for the future of Liverpool Women’s Hospital seem likely to be published before the end of the year. They will then have to go to a public consultation.
We heard on our stalls that staff at Liverpool Women’s Hospital had been told that the hospital would be rebuilt on the site of the demolished old Royal. We asked the ICB, “There is mention of a meeting with the LWH staff to reassure them about the process. Was there mention of the likelihood of funding for a new building on the Royal Site? We have been told that this happened, but this contradicts earlier statements from this board. ”
We asked the Hospitals Group board,” Regarding Women’s services in Liverpool, has the suggestion of a new Liverpool Women’s Hospital at the Royal site been raised with staff either at the Royal or LWH?“
The ICB answered. “There was a staff engagement event in February 2025. This event was to update staff on the progress and next steps of the programme i.e. the development of an options appraisal process. Consideration of the funding requirements are a part of that process for developing potential options to address the risks identified; this will be both capital and revenue costs. This was discussed in general and hypothetical terms only,as no funding decisions have been made at this point.”
We need clarity on this. If staff are being reassured by ideas of a significant new build, an idea that contradicts what the public has been told repeatedly, there is a lack of clarity.
Meanwhile, the fight to protect and improve healthcare for all our mothers, sisters, daughters, friends, lovers, and every baby continues in these grim circumstances.
Our grandparents and great-grandparents fought for and won the NHS as healthcare for all, free at the point of care, publicly provided, funded by the government, providing the best available treatment in a timely fashion. The impact of the NHS on women’s lives was profound. The NHS was won at a time of hardship in the British economy, when Liverpool and other cities were still full of bomb sites. Our current period of cuts and closures, of declining outcomes and greater birth trauma, is robbing us of the legacy left to us by the generation that defeated fascism. Fight for our healthcare like your grandparents, great-grandparents, and even great-great-grandparents. In the early 20th Century, the working-class women of Liverpool fought long and hard for better healthcare and won it. We can do that too.
Restore and Repair the NHS: June 2025; It does not have to be this way!
Last Thursday, May 29th, 2025, campaigners from Save Liverpool Women’s Hospital and Restore and Repair the NHS attended the Cheshire and Merseyside Integrated Care Board meeting. It was a truly grim meeting. The significant cuts that the ICB faces to its funding at a time of great stress to the services and our communities are a disgrace, and this lies at this Government’s feet. The blame for what this body did lies squarely with the Government, but the personal responsibility cannot be shirked.
Do not give up!
We are angry but far from giving up: “Do not appeal, do not beg, do not grovel. Take courage, join hands, stand beside us, fight with us.” (Christabel Pankhurst). Please join us and all who fight to restore and repair the NHS.
Great work goes on day after day in our NHS, but a lack of staff, resources, beds, and funding puts huge strain on the staff and damages the experience and outcomes for patients.
Problems at the ICB
The ICB system nationally is facing huge changes, financial cuts, and staff redundancies. yes the last govenment caused terrible harm. The Government has not done a risk assessment on these changes, and the impact of the Government’s financial decisions has been severe.
ICB Funding.
Hospitals are funded via the ICB. During the pandemic, hospitals were funded according to the treatments they provided. Now they must tailor their work to the money provided.
In 2024/25, the Cheshire and Merseyside ICB told NHSE it could not match the sum allocated to its planned spending. Seven other ICBs were in the same position. The Cheshire and Merseyside NHS budgets include all sixteen hospitals and primary care. Earlier in the year, they were given £178 million ‘deficit support’ ( a loan that must be paid back over several years). This was, however, still not enough to balance the books.. The ICB board met with the NHSE board, who said that if they did not balance the books/make cuts, then the £178m would be withdrawn and they would have to make £178m further cuts. The ICB must now work with each hospital to see where these cuts can be made. “On April 30th 2025 the ICB submitted a compliant plan which has resulted in both the ICB and every Cheshire and Merseyside Trust provider taking on additional cost improvement requirements (resulting in an aggregate deficit across the 16 NHS providers of c£228m offset by a surplus for the ICB of £50m.)This can be seen on page 8 of the board papers.
The ICB must also reduce its spending to meet national averages, as the area started with higher funding. Cheshire and Merseyside have the highest per-person funding, representing greater need here. But it is to be reduced over a number of years.
Wouldn’t it be good if the Government reduced poverty and ill health, too? They could start by responding to the Medact campaign for homes for all.
an Echo Photo of a protest to keep the inpatient ward in Marie Curie
The Marie Curie campaigners to keep the Woolton hospice inpatient ward open, spoke in the public questions session at the start of the ICB meeting. They spoke movingly about the need for end-of-life care, but no concrete proposals were made to save it. The responsibility is shared between the ICB and the charity.
The hospice campaign is doing such a good job,we give them our full support.
Isues at the ICB meeting
The NHS is facing harm nationally and locally. The Government and the NHS bodies are aware of this. The ICB’s finances come from the Government.
The highest risks shown in the May ICB papers are “Lack of Urgent and Emergency Care capacity and restricted flow across all sectors (primary care, community, mental health, acute hospitals and social care) results in patient harm and poor patient experience.”
Too few hospital beds and the chaos of the privatised social care system are behind the “lack of flow.”
Maternity. There have been many prestigious reports on the crisis in Maternity., many parent groups are fighting for answers. The UK has poor infant mortality rates. In England, the mortality rate for infants living in the 10% most deprived areas was over twice the mortality rate for infants living in the 10% least deprived areas. Maternal Mortality has risen “The maternal death rate increased to 13.41 deaths per 100,000 pregnancies between 2020 and 2022, according to figures published by the MBRRACE-UK investigation into maternal deaths in the UK. The figure was 8.79 in the period 2017 to 2019.” It is the highest death toll since 2003-05, when the maternal death rate stood at 13.95 deaths per 100,000.
Liverpool Women’s Hospital is featured twice in the ICB register of risks, once because it is”not compliant” financially. Although Liverpool Women’s Hospital is the centre of attention as the largest Maternity service, financial and staffing problems are shared nationwide. There is a national Maternity crisis, with Nottingham currently in the spotlight. Leeds has also reported problems following parental complaints. Wes Streeting, Secretary of State for Health and Social Care, has apologised to bereaved parents (as reported in the Health Service Journal). £100m was invested into improving Maternity safety annually following the publication of an interim report into poor care at the Shrewsbury and Telford NHS trust. However, the Royal College of Midwives reported that this national Service Development Funding (SDF) for Maternity services will drop from £95m in 2024-25 to just £2m in 2025-26. The Royal College of Midwives said, “These budget cuts are more than shocking; they will rip the heart out of any moves to improve Maternity safety. The Government has taken a wrecking ball to work that’s being done up and down the country to improve Maternity safety, something which is desperately needed.” When questioned, the ICB did not share Gill Walton’s concern. Yet Ormskirk Hospital Maternity service, one of the ICB’s Maternity providers, receives a requires improvement rating from the CQC, Liverpool Women’s Hospital requires more funding.
Our campaign to Save Liverpool Women’s Hospital is inextricably linked to the need to fully restore the NHS as a national, publicly owned, publicly provided, democratically accountable service, well-funded and well-staffed. There is a national Maternity crisis due to understaffing and underfunding. The situation for the Liverpool Women’s Hospital was not directly addressed, however, the path the ICB started on with the Engagement process last year is carrying on and that Liverpool Women’s Hospital cannot function without additional funding, but that is true of Maternity nationally. It is unclear when we will hear more of the plans for Liverpool Women’s Hospital.
Poverty and ill health. The problems in poverty, ill health and life expectancy
The Mother Statue at Liverpool Women’s Hospital
The fundamental problems are understaffing, inadequate resources, privatisation and underfunding. Few people expected the situation to continue and the issues to deepen after the Conservatives were booted out of Government. For an assessment of what the Labour Government has done, see here. We started this new Government with fewer beds and doctors per head of population than other advanced countries like France, Germany and Spain.
Labour MPs are publicising the Repairs funding the Government are giving to our hospitals but the underlying situation is a disgrace. It is a bit like an abusive husband deigning to repair the roof. The cuts to main services outweigh this, but do some MPs even know, or bother to find out?
The ICB model imposed on the NHS in 2022 is fundamentally flawed. It uses commercial rather than public service systems . Privatised public services do not work well, and mixed public and privatised health care, as we now have it in the NHS, is wasteful and damaging.
The level of funding for healthcare in the UK is inadequate and below the level provided in other advanced economies.”Among the G7, the group of advanced economies to which the UK is most commonly compared, the UK is the joint lowest spender, regardless of how we measure spend. A 2022 table puts us 37th in the international spend per head of population. Another study shows the US as the highest spender with the worst outcomes. The UK is 11th out of twelve in expenditure, but it still has better outcomes for the money spent. Our outcomes, though, are worse in cancer survival than in any country except the US. Yet they want us to emulate the US system! The Government defers to the big US companies from whom advisers and senior posts are appointed. Simon Stevens, the previous boss of the NHS under the Conservatives, came from UnitedHealth.
The ICB gives the providers (mainly hospitals) about £2,500 per annum per head of population. The level of cuts demanded by NHSE and the Government is unacceptable and will cost lives, pain and suffering.
What we learned from the ICB meeting on May 29th 2025.
“On April 30th 2025 the ICB submitted a compliant plan which has resulted in both the ICB and every Cheshire and Merseyside Trust provider taking on additional cost improvement requirements (cuts to you and me, our edit) resulting in an aggregate deficit across the 16 NHS providers of c£228m, offset by a surplus for the ICB of £50m.
Whilst agreeing a plan was essential to securing the deficit support and cash to underpin this, our attention must turn now to the effective delivery of the plan and effectively mitigating the risks.”
Risks
On Page 507, the most critical risk was “Lack of Urgent and Emergency Care capacity and restricted flow across all sectors (primary care, community, mental health, acute hospitals and social care) results in patient harm and poor patient experience, currently rated as critical,” mentioned above.
Two other risks had the highest score of 25: Elective Care and financial duties (page 550).
The ICB receives an “allocation” of money from the Government. They then must distribute that money amongst the “Providers” (the hospitals, primary care, and other services) and pay for some aspects of social care, prescriptions, services outsourced to private contractors, and private sector financial advisers like Price Waterhouse Cooper.
The NHS staff work long hours for inadequate pay and deserve much better. We thank the NHS staff and will campaign to make the NHS a great place to work once more.
Not even the poorest celiac children will now getproducts on prescription.
Marie Antoinette comes to Liverpool in 2025
Professional people making cuts that will make the poorest of families struggle to feed their families still more difficult is always disgusting, but when they ignorantly suggest people can get their essential products (such as gluten-free products for celiacs) from food banks, then the blood boils. Coeliac is a serious illness, especially for children, if not tackled by avoiding gluten foods which are up till now available on prescription. No one will use a prescription if they have to pay for prescriptions, so it’s children and less well-off people who need this. Hear our response at about one hour 37 minutes in.
Why don’t they hit the rich with their cuts? The cuts that the ICB had a choice in were cruel. They coldly and deliberately made cuts that would hurt some of the poorest in our communities, cuts that would make a slight difference to the overall budget problems. The people of Cheshire and Merseyside deserve much better. Will our area’s people passively accept this or organise to gain proper funding and an open democratic organisation of our healthcare? We say organise!
They also cut the number of fertility treatment cycles available in Cheshire and Merseyside to one. On average, it takes more than one treatment to conceive. Of course, you can have more if you pay!
Provision for long COVID was sent back to the GPs.
The scheme to take gynaecology into the GPs’ practices has been defunded.
This system of cuts is facing the ICB for the foreseeable future unless we fight like our grandmothers and great-grandmothers fought for health care.
The “winter” crisis
Cheshire and Merseyside ICB do not have enough staffing or funding to stop the winter crisis continuing into summer and through next winter. Indeed, they are expected to make further cuts. The Royal College of Emergency Medicine recently published their estimate of the number of extra deaths caused by this situation last winter; “New analysis by the Royal College of Emergency Medicine reveals that there were more than 16,600 deaths associated with long A&E waits before admission in England last year”” That is an increase of 20% (2,725) compared to 2023.
These are the issues in the “Winter crisis”. Be clear, the staff work hard and we thank them for all they do, but we do not help if we keep silent and let an unacceptable situation continue:
Liverpool Echo Photo of Corridor care
Using temporary escalation spaces to accommodate patients (corridors or even bathrooms for you and me). This is when you are acutely ill.
Waiting on trollies, rather than beds, for many hours in corridors.
Waiting “Fit it to sit” those not so sick that they are put on trollies, or if trollies are not available, being treated in chairs.
Having no access to toilets, showers, or changes of clothes.
“Boarding-in” in wards. This is where patients are put in a ward not linked to their illness and not in one of the regular beds in this ward, so not within the normal staffing levels.
Long waits to be seen by a doctor in the A&E.
Long waits for a bed once the Doctors decide to admit a patient.
Long waits for social care once treatment has been completed in the hospital.
Ambulance response times are slowed by Ambulances being stuck queuing outside the hospital.
Last winter, the situation was grim, and Liverpool Hospitals A and E had to close its doors despite the following steps: In order to free up beds, the Liverpool hospitals paid for patients who no longer needed hospital treatment to go to care homes, which provided a higher level of care than the patient needed. Arrangements were made to divert some people to walk-in centres. The public responded by not using A&E unless their condition became too severe (this can cause problems later, as treating patients at the start of their illness, rather than waiting for it to progress, is the better option). The ICB reported a dramatic drop in low acuity (less ill) cases during the highest demand period. Northwest Ambulance put on extra staff. This is emergency planning being used routinely. Yet hospitals are expected to make cuts year on year.
All of this is unacceptable, and with resources, it is avoidable.
The original model of the NHS was a national public service, publicly owned and publicly delivered, providing the best available treatment for everyone. The NHS should return to being a fully publicly provided service. We should not pay big US and UK corporations that do not improve our healthcare but leech resources from it.
Ordinary women in 1916 fought to get good Maternity care. We can fight for it too
Insurance is often proposed, most famously by right-wing parties, as a solution to the NHS’s recovery. Yet, the American healthcare system is roundly disliked by ordinary people in the USA. It also has the worst health system in the developed world, according to research conducted over many years by the American Commonwealth Fund.
We have lots of links to give more information, but the post can be read without following them.
In this blog post, we are focusing on the insurance aspect of US healthcare.
US Healthcare Insurance premiums alone cost about half of a starting salary to insure a family. (Many people pay insurance through their wages.)
Salaries in the USA
In ££
Cost of health insurance per year for a family
Single person health insurance
family health private insurance per month
Teacher (starting salary)
$50,000
£38,000
$25,000
$8,951
$2,084
Bus driver (starting salary)
$41,000
£31,000 Approx
$25,000
$8,951
$2,084
UK teachers start on £31,605 in 2025
The following are the most hated parts of that system:
Bankruptcy: Medical bills cause more bankruptcies than any other event.
Decide. The insurance company decides if you need the treatment, not you or your doctor.
Deductibles: This is the amount you have to pay before your insurance starts covering your costs. There are many payments patients have to make after they pay for the insurance premiums. “Deductibles are amounts patients pay before insurance starts covering expenses. Co-payments are fixed amounts paid for specific services, and co-insurance is a percentage of the cost the patient pays.”
Co-pays: This is like an excess on your car insurance. It’s what you have to pay in addition to the insurance for each different incidence of illness or health protection event (check-ups etc.)
Denial. You can be denied care by your insurance.
Defend. The insurance companies fight you in court if you contest their decision. They have big legal teams and it can be cripplingly expensive fight them in court.
Debt. 100 million Americans have medical debt.
Die early. Americans die earlier than in other wealthy countries
Disrespect. Giving birth costs a fortune, and more women and babies die at birth than in the UK. “25% of all stillbirths in the US are preventable today. 47% of all stillbirths in the US at 37+ weeks are preventable today.”
Fragmentationand complexity: There are many different kinds of health insurance, depending on how much you can pay. The more you pay, the better the service.
Medicines, even with insurance, cost too much, including essentials like Insulin and EpiPens.
No Cover.Some people can’t afford insurance at all.These people pay for healthcare from their own savings if they have any, from go fund me appeals, charity or go without.
Waste. Healthcare costs the US government twice as much per person as the NHS costs in the UK, despite insurance, yet it has worse outcomes for patients.
The system makes billions for the big corporations and is designed for profit.
AI,artificial intelligence data is used by insurers to say when patients should be discharged, causing real hardship.
The average cost of childbirth in the USA in 2020 was $13,383, with patients paying about $2,300 out of pocket in addition to the insurance
Infant mortality in the US is a disgrace. The UK isn’t even in the top ten, but the US is worse again.”America’s infant mortality rate of six [per 1,000 live births] is nearly 70 per cent higher than the average rate of about three for the European Union countries. And a baby born in the United States is nearly three times as likely to die during their first year of life as a baby born in Iceland, Japan or Sweden“
2022 Infant Mortality Rate: 5.547 deaths per 1,000 live births.
2022 Maternal Mortality Rate: 22 deaths per 100,000 live births.
Factors contributing to higher rates: The US has higher rates of infant mortality compared to other developed countries, with factors such as racial disparities and lack of access to healthcare.
The complexity of the US system is staggering and difficult for people to navigate. Healthcare calculations take a lot of people’s time and effort. This quote from a report to Congress shows some of the complexity.
“Private health insurance is the predominant source of health insurance coverage in the United States and includes both group coverage (largely made up of employer-sponsored insurance) and direct-purchase coverage (which includes plans directly purchased from an insurer, both on the health insurance exchanges and outside of them). In 2023, an estimated 180 million individuals (54.7% of the U.S. population) and 46 million individuals (13.9% of the U.S population)were covered by group coverage and direct purchase coverage, respectively.
In 2023, the seven big for-profit U.S. health insurers’ revenues reached $1.39 trillion, with profits totalling $70 billion.Health insurance is run to make profit not provide care. The profits are enormous. United Health reported net earnings of $420 billion per year.
The US system costs the US government more per person than the NHS costs the UK government, even though ordinary people pay a lot for their healthcare.
The federal government spent $1.9 trillion on health care programs and services in fiscal year (FY) 2024, 27% of all federal outlays in that year, and collectively the largest category of federal spending.
Forgone tax revenues to the federal government resulting from tax subsidies for employer-sponsored insurance coverage (ESI) and a portion of the Affordable Care Act (ACA) premium tax credits, together totalled $398 billion in FY 2024.
Over 80% of all federal support for health programs and services, including spending and tax subsidies, goes to programs that provide or subsidize health insurance coverage, with 36% going to Medicare, 25% going to Medicaid and CHIP, 17% going to employment-based health coverage, and 5% going to subsidies for Affordable Care Act (ACA) coverage.
In 2023, U.S. citizens collectively spent $4.9 trillion on healthcare, which is equivalent to $14,570 per person. Some of this money will be paid for patient care, some for profits, and 85% will be held in trust and invested by the insurance companies, which gives them even more financial clout than their published profits indicate .
Many in the USA call for a single-payer system. “Single-payer” describes the mechanism by which healthcare is paid for by a single public authority, not a private authority, nor a mix of both. In the USA, this would mean that the government paid everyone’s premiums, and it would be an improvement, but it is not the same as the NHS, which is more than a single-payer system.
The NHS, as it was founded, is much more than a single-payer system. The government, acting on behalf of all of us, pays for healthcare and provides it through a coordinated and integrated national system of hospitals, general practitioners (GPS), and primary care. Social care was once part of Government provision, but it was privatised under Thatcher.
The same huge corporations that have inflicicted this damage on the health and well being of people of the United States, have been invited into the NHS including those who have been penalised in the US for their behaviours.
“Centene began moving into the UK healthcare sector in 2017. In 2020 it acquired Circle Health and later AT Medics becoming the largest private provider of UK GP surgeries.
Corporate Watch uncovered that Centene and its subsidiaries have received at least £970 million in NHS contracts since 2013; £346m of this was part of a £1.57 billion COVID contract issued in 2020.
In the US, Centene is in the top ten companies with the highest penalties for government contract related offences, having paid over $1 billion dollars in fines for filing false claims.
This old cartoon from the very founding of the NHS shows that the original ideas are very strong.
The miners who organised their own health service in some of the mining towns, the women’s organisations like the Cooperative Women’s Guild, and the socialist doctors in the 1930s who fought for health care for women and babies, all built the campaign for the NHS. It was Nye bevan who as the minister in the 1945 Government brought it into being and sustained it in its early years. It is well worth reading Bevan’s own thoughts on this matter reproduced here courtesy of Public Matters.
NHS was founded to provide:
Healthcare for all, free at the point of need (the previous government changed it to be no longer free for migrants).
A comprehensive, well coordinated national service (but the ICB system breaks that up).
Publicly provided, not for profit (Lots of profits are being taken now).
Education and long-term plans for the workforce (well, it did so some time ago, now, workforce issues are chaotic).
National terms and conditions of employment (unless it’s outsourced or in-sourced).
Focus on preventative medicine and public health. Public health has been cut by 26% since 2015/16, yet in this time of climate and environment crises, pandemic and, gross poverty and poor housing we need it more than ever.
This national system has been damaged by recent governments and is still being damaged by the current one. It has been damaged by bringing in huge for-profit corporations and small-scale privatisations, and by massive cuts and underfunding and understaffing. That’s why we are fighting to restore and repair the NHS. The campaigners decades ago succeeded in establishing the NHS. If we build a big enough movement, we can do the same again; no-one else will do it for us.
At the Save Liverpool Women’s Hospital demonstration in 2023
Defend Our NHS writes”The biggest US health insurance outfit is the notorious United Health of Minneapolis[i]. Simon Stevens, a previous vice-president of this monster (now with a seat in the House of Lords), designed and introduced the destructive ICS changes with the connivance of Jeremy Hunt and without parliamentary approval“
Wes Streeting has made Samantha Jones, (a key member of the American health privatisers’ boss class), the head of the Department of Health and Social Care. Under Streeting, the NHS has told the different Integrated Care Boards to hand over the foundations of our health information to Palantir and Peter Thiel, a Trump “controller“.
We want to restore and repair the NHS on its founding principles. In that form, it was the best in the world. Cuts and austerity have severely damaged the NHS, but it is still better than the US insurance system. We need to go back to Bevan. Our campaigns fight to Restore and Repair the NHS. Please join us.
Repair and Restore the NHS for Runcorn, Frodsham, Helsby, Elton and Guilden Sutton. (This is NHS campaigners’ contribution to the debate in the Runcorn By-election and wil be upated during the campaign).
The Runcorn By-election comes at a time of anger over the state of public services including health and education, anger at the Government leaving the NHS with inadequate resouces and thereby causing deaths and making cuts at the expense of the poorest in society and those who literally need most help.
Keep our NHS Public expresses the anger (here) of most who campaign to restore and repair the NHS.
We are calling for a movement to demand the restoration and repair of the NHS. Privatisation has been a disaster for patients, staff, and the government’s spending. (Privatisation, in this sense, is the NHS paying for-profit companies to do medical work that the NHS previously provided.It’s not just charging patients)
We want, and demand this, of all the parties.
A fully funded national NHS, a fully staffed NHS, maternity care that respects and keeps women and babies safe, with no more hospital closures, a full GP service, dentistry for everyone, healthcare that manages winter well without corridor care and “boarding in“, mental health care brought back into the NHS. We want an NHS that is a good place to work. We need a good universal social care system. We want rid of privatisation and want a retun to the orginal model of the NHS without the big corporations.
Good healthcare is an excellent investment in the nation, repaying the cost in health, wealth and happiness, and financially with at least £3 return for each £1 invested. Even the world bank says “Investing in a country’s healthcare system is a strategic move that yields significant economic and social benefits, fostering a healthier, more productive workforce and contributing to overall national development and prosperity.”
The NHS was founded in July 1948 to be a national universal public service, providing the best available health care to all UK people. It was not designed to make money for big health corporations but to improve the health of the people, which it did for decades.
This model of healthcare once made the NHS the best health service in the world, in 2014 and in 2017.
The NHS was far more economical and effective than the US model.The ICB’s brought in in 2022 Act are modelled on the US Accountable Care Organisations.
The US model of healthcare is unacceptable; never mind what right wing parties say.
“The average annual health insurance premiums in 2024 are $8,951 for single coverage and $25,572 for family coverage. The average single coverage premium increased 6% in 2024 while the average family premium increased 7%. The average family premium has increased 24% since 2019 and 52% since 2014“.
Over the last 15 years, this service has been damaged by
Real-terms funding cuts,
privatisation,
enforced competition between hospital trusts,
damaging legislation (in 2012 and 2022), and reorganisation on the US model, all the time the governments are “advised” by big health corporations that preside over the worst healthcare in the advanced world in the USA.
The increasing poverty and ill health of the people.
The fabric of the hospital buildings has been neglected and we saw broken promises of new build hospitals.
Cuts in the number of hospital beds
Poor workforce planning so we have fewer doctors per head of population than other advanced countries, yet we have unemployed GPs and hundreds of doctors facing unemployment in August.
Outsourcing of services,
Services such as NHS dentistry are disappearing from many areas, and complex audiology is in severe trouble.
Commissioning medical services from private companies.
We have 6.24 million individual patients waiting to be treated, yet doctors are out of work, there is corridor care in A & E, locally we have the longest waits for admission to a ward in the country after being admitted through the A&E, and long ambulance waiting times. All this with staff overworked and underpaid. Billions are paid to outsourced for profit providers especially in mental health
We can win back the NHS
The NHS came from the people. They fought long and hard for it. From the miners of Tredegar, to the Women’s Cooperative Guild and many more, the fight for universal health care, was a long struggle. We must fight to win it back. Working class women played a big role in demanding healthcare and won some clinics but the demand was for care for everyone, from before birth to the grave and they did not stop till they won that health care. Our healthcare was never given to us by the rich. We had to fight for it.
Britain had appalling health care before World War 2. Trade Unions, especially in the mining towns, fought for healthcare for all in their areas. In some areas men were covered by workplace insurance (the panel), but not women or children. Even if a woman was employed and covered by insurance, maternity care was not included. The number of babies dying at birth was appalling, and women were more likely to die in childbirth than miners to die down the pit. Women’s groups fought for the right to health care for babies and women.
On 5th July 1948, the NHS was founded and people could see the doctor even if they had no money; there was universal access to healthcare for the first time in the UK. The health of the nation, especially children and women giving birth, improved steadily until the governments brought in austerity.
This cartoonCharley your very good health, from the founding of the NHS is interesting even today.
Attribution-NonCommercial 4.0 International (CC BY-NC 4.0). Source: Wellcome Collection.
The National Health Service linked all the different kinds of treatments, all the hospitals, all the GPs and clinics into a single organisation that allowed information and research to be shared freely.
Cheshire and Merseyside NHS coordinated campaigns are formed by Keep Our NHS Public, Defend Our NHS, Save Liverpool Women’s Hospital, local Trade Union Councils and some union branches. We call on the government to ditch their pro-privatisation policies, to fund the NHS to European levels,and to move legislation to reinstate the fully public NHS.
Please tell candidates you want to see the NHS restored and repaired. We saw the damage the conservatives did. Reform’s leader has called for an insurance model for years, and the new government has failed miserably in averting the terrible winter crisis and the Maternity crises.
For all our sisters,mothers, daughters and babies.