I am writing to you as my MP. I support keeping Liverpool Women’s Hospital at Crown Street. Please intervene to keep Liverpool Women’s Hospital fully functioning on Crown Street. I don’t care how much Spire wants the site.
As an MP, you will know about the many reports on the problems in Maternity nationally and the issues with women’s health in these years of austerity. You know about the increased risk babies face at birth in areas of poverty like Liverpool. Surely you do not support cuts to Maternity services?
The hospital needs much better funding, and all hospitals should work together cooperatively. We have a national Maternity crisis. Closing Crown Street will make things worse for all our mothers, daughters, sisters, friends, lovers, and babies.
The NHS faces an appalling winter crisis in winter 24-25. Make sure the NHS is funded and equipped to save lives, not cost lives.
Hospitals should be organised as Nye Bevan intended, a cheaper more effective system than any the Thatcherites designed.
I oppose racism. In the year we have seen the worst race riots this century, closing Liverpool Women’s Hospital at Crown Street is a slap in the face for all anti-racists. That hospital is seen as a safe space. It was built not so long ago as part of the reparations for the racism of the past.
I would like an appointment to discuss this with you.
I am writing to tell you, as my MP, just how worried I and many others, are about the situation in the NHS in Cheshire and Merseyside. We ask that you intervene.
Lord Darzi said, “The British people rely on it ( the NHS) for the moments of greatest joy – when a new life comes into beingand those of deepest sorrow.”
The current plans and lack of plans for operating with this lack of resources in Cheshire and Merseyside will damage the moments of joy and increase those of deepest sorrow.
I draw your attention to the threat to Liverpool Women’s Hospital.
I have followed the meetings of the ICB and of Liverpool Women’s Hospital. The financial situation for both organisations is unacceptable. It is wrong that the place where so many babies are born is so short of the money required to operate day to day.
The start of the process of closing Liverpool Women’s hospital, from the meeting on October 9th, is very worrying and cannot be isolated from the general crisis in the NHS. Please consider the following points
Liverpool Women’s Hospital is valued by the women of Liverpool and the public, with seventy-five thousand people signing the petition to save Liverpool Women’s Hospital. There have been three big rallies on this topic. The closure of this hospital will further damage the health of women and babies in Liverpool and the wider area. It is a regional maternal medicine centre. It is a tertiary referral centre for gynaecology, performing approximately 10,000 procedures per year. Liverpool Women’s Hospital is seen by the women of Liverpool and beyond as a safe place in an era of growing violence against women and in the context of declining health amongst women, as the parliamentary report showed
The CQC describes Liverpool Women’s Hospital as safe. Despite several recent visits, the CQC did not raise any of the issues raised by the ICB report of 9 October. Other issues related to staffing and safety in maternity were raised, but this is one of the safer maternity units in the country.
The document presented to the ICB on October 9th technically started the pre-consultation engagement about moving Liverpool Women’s Hospital services from Crown Street. Yet it gives no explanation of where our babies will be born, where gynaecology or all the other services will move to, or the indication of capital to provide alternative premises. There is no risk assessment or impact assessment.
Nationally and locally, the experience of women giving birth has deteriorated and this has done much damage. There is a maternity crisis in the UK following years of underfunding, understaffing and the disastrous outcomes of the 2012 Health and Care Act, as described in the Darzi report. It is widely anticipated that another heart-breaking report on Maternity services from Donna Ockendon will be published next month, this time about Nottingham. No one working in or around Maternity can deny the existence of this crisis. In this situation, women are angry. The CQC’s September 2024 report on the maternity service nationally said https://www.cqc.org.uk/press-release/action-needed-now-prevent-harm-maternity-services-becoming-normalised
The staffing system at Liverpool Women’s Hospital and other NHS maternity services rests on Birthrate Plus, which urgently needs review. We need better services for the babies, the mothers and the staff. Mothers and babies need more attention, and only increased staff can deliver this.
Liverpool Women’s Hospital has serious financial problems, with a deficit of 19% recently reported. The Maternity tariff on which much of their income rests is inadequate, nationally and locally. This tariff level is a core driver of the national Maternity crisis. Liverpool Women’s Hospital is currently fully staffed with midwives, at least according to Birthrate Plus, thanks to the recruitment of newly qualified staff. As with the national service, the loss of older staff who left in disgust at the safety of the whole Maternity service leaves intense pressure on these new midwives.
The health of Liverpool’s babies must have priority, especially as childhood health in Liverpool, already damaged by poverty and pollution, is not mentioned.
Liverpool Women’s Hospital is based in Crown Street Liverpool 8. It was built as part of Project Rosemary, a gesture of reparation for the terrible racism that the area has suffered. To remove the hospital in the same year as the worst race riots in Liverpool since Charles Wooton was killed is truly a slap in the face for all anti-racists.
Liverpool Women’s Hospital is one mile from Liverpool Royal Hospital; it is not “isolated.” Other branches of Liverpool Universities Hospital Foundation Trust are much further away from each other, and patients move between these buildings. The 2012 and related legislation introduced the business model, making each hospital a competing entity with other hospitals. This must change. Hospitals must work cooperatively.
One risk mentioned in the ICB document is that deteriorating women cannot be managed at Liverpool Women’s Hospital, yet the trust board has reported major improvements in this. No hospital can guarantee never having to move a patient to another hospital. About 10,000 such moves happen annually in the NHS. At present there is not a critical care unit (CCU) available at LWH. There is a high dependency unit (HDU) at Crown Street and staff working on the gynaecology HDU have undertaken training for critical care.
Another risk mentioned in the document is that other hospitals in Liverpool do not have staff to deal with pregnancy or other gynaecological conditions. This must be addressed, but not by closing Liverpool Women’s Hospital.
Another risk mentioned is that services might be moved out of Liverpool if certain specifications are not met. But this report does not say where Liverpool’s babies will be born. Will that, too, be sent out of Liverpool?
Risk 4 discusses recruitment and retention difficulties. Midwives at LWH face no recruitment problems. The problems with other specialities are national, not local.
In the weirdest contradiction, Risk 5 says, “Women receiving care from hospital services, their families and the staff delivering care may be more at risk of psychological harm due to the current configuration of services.” Closing Liverpool Women’s Hospital will definitely risk psychological harm, as the place we see as safe is taken from us against huge popular opposition.
The engagement events are inadequate. Only two of these events are not in working hours, none are in North Liverpool or locally in central Liverpool. It requires time and some computer skills to register for them.
I also have serious concerns about the NHS winter crisis 2023-24, which the ICB has been clear will not be better than last year. The ICB is underfunded ( but spends too much on financial consultants and contracts, driven to do so by NHSE.) It is also under pressure to get the Liverpool Specialist Hospitals, Liverpool Heart and Chest, Liverpool Walton Centre and Clatterbridge Cancer Centre firmly into the cash-strapped ICB control. Liverpool Women’s Hospital is also partially funded through the specialist hospitals programme and is affected by this move from national to local funding.
I recall the announcement nine years ago that one Liverpool Hospital must close, and then it was announced that Liverpool Women’s Hospital was the one they had chosen. The chaos over Liverpool Royal New build and PFI, plus the pandemic, gave some breathing space, but the coming of the ICB and NHSE’s determination to reduce the number of hospitals in Liverpool have brought this back to the table.
I would like to discuss this with you personally.
For all our mothers, daughters, sisters, friends, lovers and babies, Save Liverpool Women’s Hospital
These are notes from Lesley Mahmood and Sheila Altes, who gave the first responses to the proposals from the public presented at the ICB meeting on October 9th 2024. A more detailed response is being prepared. The ICB is the “Integrated Care Board” the big bosses of the NHS in Cheshire and Merseyside. You can find their papers here. The recording does not show the questions and contributions from the public but you can see some of those contributions on another post on this blog.
Points & questions for the ICB’s public meetings
(ALWAYS SAY YOU WANT YOUR COMMENTS NOTED IN DETAIL)
HOW & WHEN HAVE THESE PUBLIC MEETINGS BEEN ADVERTISED TO THE PUBLIC?
“I want to question the whole basis of this meeting, this process and the nature of this ‘consultation.’
“Losing LWH at Crown St has been the ambition of NHS decision makers since March 2015 when the then chair of the CCG on Panorama stated Liverpool has too many hospitals & 1 has to go. The Echo had a story about it the day before. The day after the Panorama programme, the Echo’s lead story was the Women’s Hospital to close. That’s when our campaign started.
This 2024 ‘proposal’ is against the backdrop of closures of hospitals, A & Es, 1,000s of beds up & down the country. Some of these same decision makers told us that the Royal PFI/Carillion build with PFI & 300 fewer beds, a smaller A& E would meet the needs of Liverpool. Instead, we had massive debt, delays, A& E overwhelmed, 12-hour waits, and corridor care.
Why avoid saying what’s to become of the Crown St site (on p.109 of the ICB document)?
In the last 12 months the ICB has indicated that £150m+ for an equivalent new build on the site of the old Royal is ‘unlikely’ ‘n the next 10 years. £150m is the deficit of the ICB. In Cheshire & Merseyside, Leighton is the only likely new hospital, which is falling in due to its crumbling concrete.
So where’s the capital ( the money for buildings and costly equipment), or will we have 1 or 2 small Maternity wards tacked on somewhere? This will cause the ethos of the Women’s Hospital to be lost.
What will replace LWH at Crown St? It’s not good enough to say it will be used by the NHS; who will provide them, private companies like Spire/ Spa Medica? Under the Naylor Report, surplus’ and not fit for purpose NHS buildings or land is to go up for sale. We have been told by staff in Spire that Spire is very interested in Crown St.
Why should a £15m new neonatal unit & a new scanning unit of several £m be scrapped?
Women in Liverpool 8 & beyond regard LWH at Crown St as a safe space, a green space (good for recovery & mental health), a low rise, easy to get into in an emergency, especially valued by the L8 community, who regarded the LWH being developed at Crown St as part of Project Rosemary after the Toxteth Uprising of 1981 as some compensation. The wife of the Dean of Liverpool signing our petition recently said -he was 1 of the people responsible for Project Rosemary. The LWH is also valued by the other 75,000 people who have signed our petition.
There’s no mention of the positive impact of LWH being based at Crown St. On p.107, it is claimed that Crown St means worse gender inequality. Where is the evidence for this? On p.63, for instance, the maternal mortality is in line with national data and where is the equality impact assessment referred to on p.110?
The ICB document talks about 5 risks at Crown St, I want to question these.
RISK 1. Acutely deteriorating women cannot be managed onsite at Crown Street reliably, which has resulted in adverse consequences and harm.
( We know this experience can be horrible for the women involved)
The paper cites the cause as a lack of onsite services and specialist staff, e.g. critical care, medical and surgical specialities and 24/7 blood transfusion labs. At present, there is not a critical care unit (CCU) available at LWH, but there is a high dependency unit (HDU) at Crown Street and staff at the gynaecology HDU have undertaken training for critical care.
The Core Standards for Intensive Care Units (2013) state that it is preferable to have an intensive care unit on site, but units without such a provision must have an arrangement with a level 3 CCU and a policy for the safe transfer of patients when required. LWH has such an arrangement with the Royal Liverpool University Hospital (RLUH) which is situated 1.3 miles away.
A lack of medical and surgical specialities was also cited. A Medical Emergency Care Team is being recruited to enable optimal care and transfers if necessary. LWH is also participating in the “deteriorating patient collaborative” to improve earlier recognition of clinical deterioration. There are clinical pathways in place for the acutely unwell/critically ill pregnant or recently pregnant woman. Women with complex needs are seen at specialist clinics, where a consultant obstetrician and consultant in the relevant specialism will plan the treatment necessary to ensure optimal care. LWH is the recognised provider of high-risk Maternity care and complex gynaecology procedures in Cheshire and Merseyside. Emergencies will inevitably occur, and a transfer to a CCU will be needed. Inter hospital transfers of critically ill adults take place frequently, it is estimated that 10,000 of such transfers take place annually in the UK (BJN 22/04/21).
A 24/7 Blood Transfusion lab is to be developed at the Crown Street site. As well as the extension of some laboratory services.
Given all of these developments and the small number of patients being transferred to CCU (see page 46 of the Case for Change), why does the ICB consider co-location necessary, especially in a time of financial restraint?
RISK 2: When presenting at other acute sites (e.g. A&E), being taken to other acute sites by ambulance or being treated for conditions unrelated to their pregnancy or gynaecological condition on other sites, women do not receive the holistic care they need.
Board papers state that the risk is caused by a lack of women’s services and specialist staff at other sites in Liverpool. However, it is difficult to see how re-location would solve this if LWH is re-located to the RLUH; women are still likely to turn up at the Aintree site and vice versa.
Is the ICB looking at Maternity and gynaecology services at 2 different sites? How will this fit with LWH as a Maternal Medicine Centre (MMC)?
LWH has its own Emergency Department with much shorter waits than the Royal/Aintree A&Es, if LWH is moved, will its Emergency Department close and women have to queue up in the general A&Es?
This dispersal of services would not fit with the ethos of a specialist hospital for women, and that surely would be a gender inequality, as women’s health differs from that of men in many unique ways. It is influenced by biology and conditions such as poverty, employment and family responsibilities. Women’s reproductive and sexual health have a distinct difference compared to men’s health. (Cardiovascular disease, common to men and women, can lead to pre-eclampsia in a pregnant woman. Sexually transmitted infections can cause such outcomes as stillbirth or neonatal death. Other issues impacting women’s health include unplanned pregnancy, non-consensual sexual activity, domestic violence and female genital mutilation). Centres of excellence in women’s health, such as LWH, can advance research and large-scale clinical trials to address these issues, but the dispersal of services cannot.
RISK 3: Risk 3: Failure to meet service specifications and clinical quality standards in the medium term could result in a loss of some women’s services from Liverpool.
Maternal Medical Centres (MMC) are responsible for ensuring that all women on the network’s footprint with significant medical problems will receive timely specialist care and advice before, during, and after pregnancy. LWH has been selected as one of 3 MMCs within the North West, along with St. Mary’s Hospital in Manchester and the Royal Preston Hospital in Lancashire. The model of care ensures that the highest risk and most complex women will have most of their care delivered by the MMC.
No hospital in the UK is equipped to deal with every eventuality. Therefore, it is inevitable that patients sometimes have to travel outside their area.
At present, women with complex congenital heart conditions are sometimes treated in Manchester. The RLUH cannot deal with some complex bowel surgery, and patients sometimes have to travel to the Christie Hospital also in Manchester. Yet, there are no questions about relocating the Royal, so why the Women’s Hospital?
Risk 4: Recruitment and retention difficulties in key clinical specialities are exacerbated by the current configuration of adult and women’s services in Liverpool.
Recruitment and retention of staff is a national crisis in the NHS as a whole and not just in Maternity services.
There has been a 9-year threat to reconfigure services at LWH, which may have hurt recruitment.
As a teaching hospital, LWH is a centre of excellence in the provision of undergraduate and postgraduate medical education and training. LWH has a highly active multidisciplinary research programme that includes research into Maternity studies, gynaecology studies, fertility studies, genetics, oncology and neonatal studies.
The claim that the difficulties in recruitment are caused by an inability to provide comprehensive multidisciplinary team working and training on acute sites makes Liverpool Women’s Hospital a less attractive place to work is hard to believe. We favour joint appointments and joint working to provide comprehensive training and development opportunities.
Governments have deliberately reorganised and underfunded the NHS. There is a national Maternity crisis. Maternity nationally has historically been underfunded through the Maternity tariff. This affects LWH particularly. So, fund it, don’t lose it!
RISK 5: Women receiving care from hospital services, their families and the staff delivering care may be more at risk of psychological harm due to the current configuration of services.
In a time of increased misogyny, violence towards women and austerity policies that disproportionately affect women, LWH is seen by all women of all ethnicities, as a safe place for women.
For the last 14 years, NHS staff have been underpaid, overworked, and undervalued, conditions exacerbated by the pandemic that still continue. The Ockenden review highlighted these issues throughout the country, so psychological problems are not exclusive to the Women’s Hospital.
In a recent staff survey for the LWH Board, 49% of staff feeling negative about their work said they felt overworked. (p.24 People Pulse report, LWH Board papers 10.10.24)
Ockenden called for more staff, more midwives, and more Maternity funding. We need more midwives & we need to keep experienced midwives to support newer midwives.
On the 9th and 10th of October, there were two developments about Liverpool Women’s Hospital.
The Integrated Care Board, the funding and organising body for Cheshire and Merseyside NHS, agreed to start the process that can lead to the closure of Liverpool Women’s Hospital. We think this will damage care for women and babies. We have had enough of hospital closures and shortages of hospital beds.
The final meeting of the Liverpool Women’s Hospital Board was held. In future, the decisions about LWH will be made at a joint meeting of the board of Liverpool Women’s Hospital Trust and the board of Liverpool Universities Hospital Trust. Behind this is the appalling state of finances for maternity care nationally, especially for Liverpool Women’s Hospital, the largest Maternity provider in the country.
While these changes are being debated, the Women’s Hospital stays on the Crown Street site and continues functioning.
You have a right to say “No.” Never forget that right to say NO!
The NHS must listen to the people. We need your voice. These proposals do not discuss finances, nor do they discuss where our babies will be born in future or what will happen to the current Liverpool Women’s Hospital site on Crown Street. They just legally clear the way to close Liverpool Women’s Hospital.
Liverpool Women’s Hospital is where most of Liverpool’s babies are born. It is the largest centre for Cheshire and Merseyside for gynaecology and women’s health. It also provides other services in a good building on a pleasant green site. Liverpool Women’s Hospital has far less traffic around it than does the new Royal. One of the reasons given for closing Liverpool Women’s is that other hospitals don’t provide safely for women who happen to be pregnant. Those hospitals should be improved, not used as an excuse for closing Liverpool Women’s Hospital.
NHS England wants all hospitals in the envelope of the ICB system rather than having specialist hospitals with favourable specialist funding given nationally. This affects The Heart and Chest Hospital at Broadgreen, the Walton Centre and the Clatterbridge Cancer Centre. This follows the US Accountable Care Model.”Accountable care organizations (ACOs) were created to promote health care value by improving health outcomeswhile curbing healthcare expenditures” They were designed for healthcare provided by private for-profit corporations, not for a public service system like the NHS.
Within Cheshire and Merseyside ICB, there are “Places” These places are the groups of NHS services within each local government area. Liverpool Place is responsible for all these hospital reconfigurations even though each hospital serves an area wider than Liverpool.
According to many different reports and our own experiences, we have a Maternity crisis and a crisis in women’s healthcare. NHS problems, though extreme for women, are not exclusive to Maternity and women’s health care but extend to A&E, the GPs, dentistry, mental health, the considerable waiting lists for treatment and much more.
We are holding a workshop at 7pm on Monday 14th October at the Quaker Meeting House School Lane Liverpool behind Primark in the city centre. It will also be available via Zoom. Please register here. You do not need to be an expert to come to this workshop; you just need to be a human who cares about safe healthcare as public service or is interested in the issues.
The ICB is in financial difficulty caused by underfunding and by money sucked out through privatisation. Below is the ‘heat map’ of risks facing the Cheshire and Merseyside ICBs. Black 20 is the highest risk level. This is from the ICB public papers for the September meeting.
Maternity and women’s health have been underfunded and under-staffed for the whole time the Conservatives were in office. This must change. We did kick that government out. Remember?
We need improvements at Liverpool Women’s Hospital and the other hospitals in Merseyside and Cheshire. We need funding for the winter crisis. The prospects for the winter crisis look bleak. The ICB should be spending money on the winter crisis and improving our services, not closing services.
The ICB will hold public engagement meetings in the next six weeks about the ICB’s plans to close Liverpool Women’s Hospital. As we write this, we have no idea where or when the meeting will be held. Please do go to these meetings if you can. Do not be afraid to say NO!
The whole NHS is in crisis. The general election has not (yet!?)solved this situation for the NHS. It is still underfunded and still being restructured toward final privatisation.
The winter crisis is set to be worse than last year’s estimated 300 excess deaths per week. People will have more pain and more time being unwell. More people who would not otherwise die will do so unnecessarily. Yet all of Liverpool, Merseyside and most of Cheshire voted Labour. Tell your MP to solve this situation to stop the damage to the NHS. They have the power to do so if they have the political will.
There is a significant difference between the management of the NHS nationally and at the Integrated Care Board level and the work of NHS staff who treat us as patients. We can disagree with NHS bosses and national, regional, and ICB managers without disrespecting the NHS workforce, doctors, midwives, nurses and all the other roles in the NHS who do great work under challenging conditions.
Do not wait until the winter or Maternity crises hit your loved ones.
Join us in the campaign to Restore and Repair the NHS.
What you can do
Talk to your friends, family and workmates about the NHS. Every powerful campaign starts with talk.
Remind people that health care strengthens an economy and makes people healthier and happier. No economy can be strong with millions unable to work while they wait for treatment. We must afford good health care for all our mothers, daughters, sisters, friends, lovers and all the babies. Each person is born just once. We have to make birth as safe as humanly possible, which is safer than the UK currently manages. The UK are 18th in the safety ranks. Once we were up at the top.
Go to the so-called public engagement meeting the NHS is organising to sweet talk you into agreeing with their cuts and tell them what you think; don’t just be disgusted; tell them so!
Raise the state of the NHS with your union. This can be powerful.
Email your MP or get an appointment to see them.
Talk to your councillor. They have a role in this through the Place Partnership board.
Sign our petition.
Help our campaign! Help distribute leaflets, posters, banners, and social media posts.
Today, October 9th 2024, the ICB started the legal process that will allow them to close Liverpool Women’s Hospital. The papers for this meeting can be found here. Campaigners opposed the plans. We include videos of some of the contributions in this post.
Protestors outside the ICB meeting discussing the future of Liverpool Women’s Hospital.
The document did not discuss the financial situation or alternative provisions, nor did it include an assessment of the benefits of having a stand-alone Women’s Hospital.
After decades of cuts in healthcare and growing crises in women’s health and Maternity, there is naturally great concern about these plans. Similar plans have been put forward before. Seventy-five thousand people have signed our petitions to keep Liverpool Women’s Hospital open, and we have held three large demonstrations over its future.
Act now to avoid the winter crisis, with patients dying because of the long waits.
Keep Liverpool Women’s on the Crown Street Site and staff it well, with all the specialisms required to improve care and minimise transfers out of LWH. Give it long-term security.
Improve the intensive care at Liverpool Women’s Hospital.
Make all hospitals work cooperatively, not as competing organisations.
Protect the Emergency Departments at Liverpool Women’s Hospital.
Provide emergency Obstetric and Gynaecological care at the A and E at the Royal and Aintree.
Nationally, address the workforce training issues that have resulted in shortages of key roles, like anaesthetists.
Make the NHS a great place to work.
Act against the racism that damages the health of women and babies health.
Protestors holding a small sample of our petitions.
Liverpool Women’s Hospital opened in 1995. It is a modern low-rise hospital on a garden site in good condition. It provides maternity care and gynaecology for most of Liverpool’s women. About seven thousand babies are born there each year. It has a new large neo-natal unit and provides other linked services. It is just over a mile from the Liverpool Royal Hospital site.
Lesley Mahmood for Save Liverpool Women’s Hospital.Part one
The second half of Lesley’s speech
The ICB (Integrated Care Board) now runs finance and planning for the Cheshire and Merseyside area of the National Health Service, one of 42 such areas in the country, following the 2024 Health and Care Act. The aim is to bring all health spending for the area into this body and to restrict that spending. This mimics the Accountable Care boards that operate in some US States or cities. In the US, these organisations comprise one big or several small private healthcare corporations providing healthcare for profit. The Government provides funding, and the corporation profits by restricting the service. There has been a revolving door between the leaders of the NHS and the big US health corporations for some time, and there are close links between the governments and those big US health corporations. For details, see here.
This is an American definition of ACOs. “Accountable care organisations (ACOs) are defined as groups of clinicians, hospitals, and other healthcare providers who work together to provide high-quality, coordinated care to a defined population. If an ACO meets quality standards, achieves savings, and meets or exceeds a Minimum Savings Rate, the ACO will share in savings based on the ACO quality score.“
Felicity Dowling speaking for Save Liverpool Women’s Hospital Campaign.
The very grave financial difficulties of the NHS, this ICB, and Liverpool Women’s Hospital were not discussed. It was presented as a purely clinical case – as though such an idea is possible in such a funding crisis for the NHS. The Liverpool Women’s Hospital has been structurally underfunded for many years. The Maternity tariff and Birth rate + are inadequate. This funding problem affects all Maternity units nationally. Still, the impact is starker at Liverpool Women’s because it is such a large Maternity unit and does not share its budget with a general hospital. The Government made up some of the difference until the ICB was formed two years ago, but that has ceased. Many of the very real problems at Liverpool Women’s over the last few years stem from this chronic underfunding.
Greg Dropkin speaking at the ICB meeting. Greg is from Keep Our NHS Public.
Today’s meeting will be followed by a public engagement period, during which the public might be allowed to contribute to the discussion.
We believe Maternity is massively underfunded, and that is at the core of the national maternity and birth trauma crisis.
There were no alternative plans put forward as to where our babies will be born or where women’s health care will be delivered.
The core case made was that the most severely ill patients have to be transferred to the Royal, one mile away, and that women with obstetric and Gynaecological issues who present at the big A & E do not have on-site obstetric or gynaecological care available at those big sites.
Protestors reminded the board that the plans to close one hospital in Liverpool date back to 2015 when the then-head of the Clinical Commissioning Group announced them on a panorama programme.
Sheila Altes responded about some of the risks in the document.
Save Liverpool Women’s Hospital 2024 for all our mothers, sisters, daughters, friends, and lovers and for all the babies.
The ICB meets on Wednesday, October 9th, to put forward its latest attempt to close Liverpool Women’s Hospital.
Without the long and publicly promised consultation, before proposals were made, the ICB is determined to close our much-needed hospital.
Our campaign rejects any attempts to close, merge, disperse or cut services for the women and babies of the whole area. None of the half-suggestions in the papers will improve anything for women or babies.
Such papers are impossible to evaluate without a financial statement, research background, and impact assessment, all of which are missing from the proposals.
The financial background for the whole NHS is grim. The last government’s financial plans and policies are still in place. The ICB in Cheshire and Merseyside is in severe financial trouble. There is a looming winter crisis. NHS England has said that the trusts must squeeze staff costs, and there is no chance to surge extra beds and social care resources as they did last year. We have consistently challenged the ICB on this.
Liverpool Women’s has structural financial problems. The largest maternity service in the country is most impacted by the inadequate Maternity tariff. Financial problems are not mentioned in the paperwork. No other hospital can improve on the Liverpool Women’s Hospital maternity service without improved funding.
Proposing to close our hospital in the traditionally Black area of Liverpool, in an area of hardship, just weeks after the worst examples of racism the city has seen in decades is disgusting.
Save Liverpool Women’s Hospital 2024 for all our mothers, sisters, daughters, friends, and lovers and for all the babies.
The ICB meets on Wednesday, October 9th, to discuss its latest attempt to close Liverpool Women’s Hospital.
Without the long and publicly promised consultation, the ICB has gone ahead, determined to close our much-needed hospital.
Our campaign rejects any attempts to close, merge, disperse or cut services for the women and babies of the whole area. None of the half-suggestions in the papers will improve anything for women or babies.
Papers such as those published for the meeting on October 9th are impossible to evaluate without a financial statement, research background, and impact assessment, all missing from the proposals.
The financial background for the whole NHS is grim. The last government’s financial plans and policies are still in place. The ICB in Liverpool is in serious financial trouble. There is a looming winter crisis. NHS England has said that the trusts must squeeze staff costs, and there is no chance to surge extra beds and social care resources as they did last year. We have consistently challenged the ICB on this.
Liverpool Women’s has structural financial problems. The largest maternity service in the country is most impacted by the inadequate Maternity tariff. Financial problems are not mentioned in the paperwork. No other hospital can improve on the Liverpool Women’s Hospital maternity service without improved funding.
Liverpool Women’s Hospital needs a level 3 high dependency unit added to its Intensive Care provisions, and it needs some more specialist staff, all of which would be more efficient and equitable than the current semi-proposals.
We will not stand by and see women’s services sacrificed again.
In 2015, plans were set out to close one Hospital in Liverpool, and they chose to damage services to women.
Liverpool Women’s Hospital’s financial problems are caused by the poor funding of maternity nationally, and the cost of the foundation trust system.
Maternity and women’s health need urgent changes, but these don’t include dispersing services and absorbing Liverpool Women’s Hospital into one giant conglomerate. Should we leave structural issues in our health care to “the professionals”? No way. The big managers of the NHS have caused havoc in the last ten years, implementing austerity, privatisation, the chaos of the building of the new Royal, and the move towards an American healthcare model. We have seen more than a decade of damage.
The priority must be the health and well-being of the women and babies of Liverpool. For too long, women and babies have paid the brutal price of austerity and poverty.
The ICB say they think it will help poor and black women to move a hospital from Crown Street, in one of the most hard-up areas of the city, and the traditional Black centre of the city! This within weeks of the most serious organised racist attacks in the city in decades.
We have always said hospitals should work cooperatively, rejecting the 2012 Health and Social Care Act competition model.
75,000 people have signed the petition to save Liverpool Women’s Hospital. There have been three large rallies, and countless meetings and street stalls on this issue.
Only the hard and skilled work of NHS workers and in this case especially, midwives, have kept a service afloat.
Restore and repair the NHS! Save Liverpool Women’s Hospital!
Liverpool Women’s Hospital is a much valued service for women and babies. The history of the building and the site are important, especially as racism has reared it head in Liverpool in a way unseen for decades. It is a modern low-rise building in good condition. No wonder the private sector lusts after it. The Crown Street site is, importantly, a green site, which helps sick women and babies heal, which is good for babies’ lungs, and is a good place to be born.
Nationally, Maternity is badly funded and badly organised. The Government spend more on payouts from the insurance than for the whole service. There has been a flight of older, more experienced midwives from the service, making the work of our much-valued younger midwives harder. Midwives nationally have been clear about the dangers, and a slew of reports have shown the damage done to women and babies. All these cases have been in co-located maternity systems.
NHS workforce planning has been appalling in the last decade. Blaming a standalone site for workforce shortage is ridiculous. The situation for anaesthetist training is a national scandal.
We call on the city of Liverpool, Merseyside, and beyond to defend what we have in the NHS, and to fight to improve the rest. No closures, no loss of services, no more mergers, no more outsourcing, no more overworked staff.
What has Liverpool’s “Place” NHS and Cheshire and Merseyside ICB done whilst maternity care nationally is in a well-publicised crisis and thousands of women are furious about the level of care they and their babies received? While the public enquiry into baby deaths at Countess of Chester has just opened? While Alderhey is at the centre of the Physician Associates scandal? While they can’t stop the next winter crisis, already upon our hospitals?
They announce the intention to fundamentally change Liverpool Women’s Hospital. This was without even a meeting with the organisations that have campaigned for a decade to keep the hospital and collected 75,000 signatures to keep the hospital on the Crown Street site as a women’s hospital for all our mothers, daughters, friends, lovers and for every precious baby.
The whole ICB is facing huge problems and does not have the resources to deliver safe A and E in the coming months. Yet, they think launching a discussion about merging Liverpool Women’s Hospital into one conglomerate of hospitals is sane and responsible.
This is the state of the Integrated Care Board, which is the controlling body for the NHS in Cheshire and Merseyside. It is from page 110 in the Board papers. A score of 20 in black means it is at the highest risk possible. They also said:
“There are currently no known plans for any additional funding to be allocated ahead of winter to support additional capacity and the expectation is that maintaining system flow through winter will need to be achieved through the delivery of these improvement plans.“
The document about Liverpool Women’s Hospital’s future can be found here. We will produce a detailed critique next week.
Maternity and women’s health need urgent changes, but they don’t include dispersing services and absorbing Liverpool Women’s Hospital into one giant conglomerate. We want to see the following changes nationally and locally.
Far better funding and staffing for maternity and an end to birth traumas.
More respect must be given to women giving birth and the women tending them in giving birth.
The funding currently given to insurance for maternity damages should be invested in the service to reduce those damages.
Women who need induction of labour should get that intervention in a safe and timely manner.
Fertility services must be fully available on the NHS, not the prerogative of the well-off.
Gynaecology services must be drastically improved, nationally and locally.
The NHS workforce must be given more respect, their workload improved, and the service must once more become a good place to work.
The whole NHS must be returned to being a national, fully publicly provided service, fully funded, repaired, and restored after all the damages of more than ten years of austerity and many forms of privatisation.
The public’s views must be respected – most women likely to use the hospital will be at work when this first meeting happens.
The research conducted at Liverpool Women’s Hospital must continue into key areas like endometriosis, menopause, and working to ensure our prem babies live and thrive despite being born very early.
Midwifery training must be made available to all without incurring huge debts.
Women’s health and healthcare must be given far more resources and respect.
Our petition, which is available on-line is at 44,656 signatures and more than 30,000 signatures on paper, says “Save the Liverpool Women’s Hospital. No closure. No privatisation. No cuts. No merger. Reorganise the funding structures not the hospital. Our babies and mothers, our sick women, deserve the very best”
It has over seventy-five thousand signatures. The people of Liverpool have attended three big demonstrations to save the hospital. Campaigners have attended every board meeting of Liverpool Women’s Hospital since the petition was launched and every ICB meeting since that was formed. Yet we have never been invited to present our views. Promises of consultation made in public clearly meant nothing.
Twenty thousand signatures were presented to the ICB in January 2023
Liverpool Women’s Hospital is a tertiary centre, which means patients are referred there from other hospitals from the rest of Merseyside and Cheshire, the Isle of Man and parts of Wales. Keeping that provision and the reputation that goes with it is important. The provision for the babies in the neonatal unit, near their mums, matters too.
We have said for years that the NHS must change the maternity tariff, the amount of money paid to hospitals for delivering maternity care. Liverpool Women’s Hospital is the largest provider of maternity care and is badly hit by how low the tariff is. Liverpool Women’s Hospital runs a deficit because of this, and over the years appears to have made some bad decisions on staffing because of the financial problems. Many midwives left. Yet somehow,the document from the ICB says:
“The case for change is focussed solely on the clinical risks, issues and outcomes for people using hospital-based gynaecology and maternity services. It does not consider productivity or value for money.”
The ICB is in serious financial trouble yet it claims not to be considering money in this situation.
We say that right from the beginning, it has been about money. It was about the decision made nearly a decade ago to close one of the Liverpool Hospitals to save money at the cost of our health. It is also about disrespecting women’s health and women’s opinions.
“We’ve known for some time that the poorest households and women have shouldered the greatest burden of austerity measures.” Women’s health has suffered particularly in this time. Liverpool has seen some of the worst overall loss of healthcare. Yet we still kept Liverpool Women’s as a treasured service, where most of Liverpool’s babies are born and where great steps have been made in research. We said before and say it again “In these hard times. what we have we hold.”
Should we leave structural issues in our health care to “the professionals”? No way. The big managers of the NHS have caused havoc in the last ten years, implementing austerity, privatisation, and the move towards an American model. We have seen more than a decade of damage.
Remember the chaos of the building of Liverpool Royal, with fewer beds than the old one and now needing more, with chaos in the financing, construction, and demolition?
We call on the city of Liverpool to defend what we have in the NHS and to fight to improve the rest. No closures, no loss of services, no more mergers, no more outsourcing, no more overworked staff.
We do not accept that our children should go hungry and that our elders must suffer from the cold this winter. Both are wrong and both policies will increase pressure on the NHS.
Our NHS is a matter of life and death, (and the working class die first).
Good healthcare makes a country healthier and wealthier. No country can thrive with poor healthcare. No country should have millions unable to work due to a lack of health care.
Healthcare is a human right. The generation that defeated fascism gifted to us, their descendants, the best system of healthcare in the world. This was according to the US Commonwealth Fund. We are now ranked 10 out of 11. We want our inheritance back. No ifs no buts.
The NHS has been bled dry by privatisation, by bringing in the market into healthcare, by austerity and cuts to real term funding, by appalling workforce planning, by letting maternity as a service decline, by the frightening damage to our mental health service, by cuts to beds and inadequate staffing and by the neglect of the fabric of our NHS buildings. These have all caused grave harm some of which the Darzi report mentions.
But each problem can be reversed by government policy if they so choose. These were policies of the Conservatives. They must not be the policy for Labour too.
Professor Danny Dorling has just exposed the cruel cost of austerity to our children. Our children have been hurt more than any other nation by years of austerity. They are becoming smaller in size,bringing back stories of how in world war one too many men were too small,too stunted in size, by poverty to fight. There must be a full break from this to allow our children to thrive.
Our NHS staff work hard and with great skill, kindness and talent but they cannot cope with this imposed poverty of resources, disorganisation and crumbling buildings.
Mothers are describing traumatic birthing experiences in numbers to big too ignore.Midwives report the problems in the labour wards and in ante-natal and post-natal care. We don’t need to repeat the evidence already given in numerous reports, from respected organisations.
Mr Starmer ( a Labour prime Minister) is refusing to respond to the emergency on our doorsteps this winter until a set of “reforms” are introduced.
Mr Starmer says his priorities are digitisation, ( Lots of money there for the big tech companies but we need midwives.) moving care out of hospitals and producing a healthier population.
We urgently need a publicly owned, not for profit, user designed social care system.That will take huge political will and investment but would make so many lives better. Is this too much for us Mr Starmer?
The government must choose to invest now to achieve vital short-term and long-term goals in our healthcare. They must also design our health care as a public service, not a pig’s trough for the rich to root in for tasty morsels. Governments spent five times the cost of the NHS on Quantitative Easing, they spent billions on the Bankers’ crisis, and they are spending billions on the war in Ukraine. See this article for more on Government spending. The NHS too is a crisis that the government must tackle The last government got hammered in the General Election for its policies. Following the same policies will get the same response.
There must be urgent action.
What are we supposed to do in the meantime? Die quietly? Suffer silently? Sit in pain, and get worse for hour upon hour in A and E? Should we be silent while staff are underpaid and overworked? We need action now before this winter’s crisis kills more of us.
We need action on maternity. Mothers in labour cannot wait. We know all we need to know about how bad the situation is. The reports are numerous. Women and babies need action now.
The GP service is badly damaged and the GPs need a positive response from this government now. All private companies running GP surgeries should be removed. Every available GP should be employed.
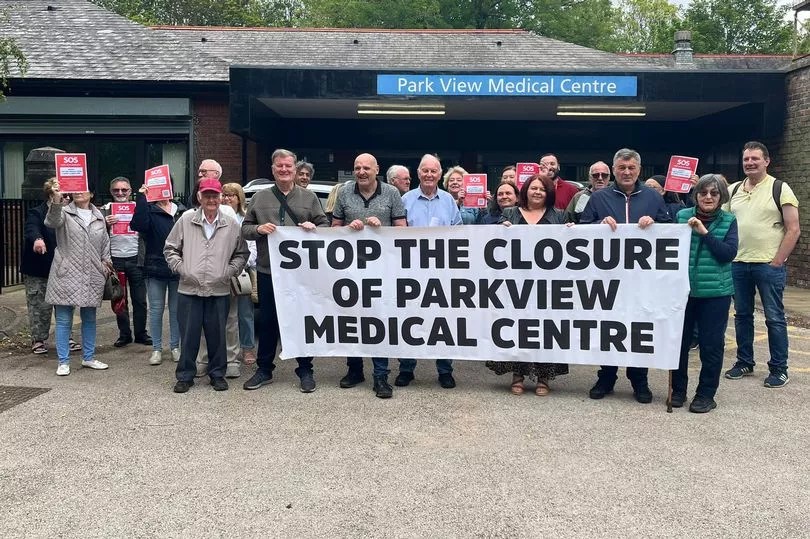
Park View patients protesting the closure of their GP Practice
Patients live longer with consistent access to a GP. The appalling statistics for life expectancy, an life expectancy in good health in poorer areas of Britain make this especially important. In Liverpool the gap in life expectancy between richer and poorer areas is large and the “rich” areas of Liverpool are far from the richest in the country “Life expectancy at birth in Liverpool, is 76 years, although this masks variation, with an average of 76.4 years in Anfield and Everton compared to 83.1 years in Childwall and Wavertree.”The Office for National Statistics said
In 2018 to 2020, male healthy life expectancy (HLE) at birth in the most deprived areas was 52.3 years, compared with 70.5 years in the least deprived areas. Female HLE at birth in the most deprived areas was 51.9 years, almost 20 years fewer than those living in the least deprived areas (70.7 years).
Mersey Pensioners protesting about Physician associates being used instead of fully qualified doctors.
We say
Fund and organise action now to improve the situation for this coming winter, including lifting financial restrictions, opening more beds recruiting staff, make more space available.
Improve maternity funding immediately so hospital managers are not pushing staff to cope with too few resources, and too few staff. Improve the maternity tariff. Improve the ratios of midwives to birthing mothers. Bring back health visitors. Tackle infant mortality. Try to win back some of the staff who have left in disgust at the poor state of maternity. Heed what women are telling you about maternity. Stop the epidemic of birth trauma
Save Liverpool Women’s Hospital, the largest in the UK. No to mergers.
Employ more GPs not less qualified substitutes. Kick US corporations out of our GP practices.
Let’s get back to a national, publicly provided health care, for all, free at the point of need. The poison of privatisation, outsourcing, insidiously introduced charging and the business model has done great harm.
Our health records are and must be private. We know there is huge value and potential profit in the data to be obtained from a large and well-established national health service but that wealth belongs to the people, including the poorest of us. Use only an NHS digitalisation system agreed with doctors and nurses. No external system owned by dubious US corporations should be allowed near the NHS. We saw what Fujitsu did to the sub-postmasters.
You can help.
Photo from the Liverpool Echo of Liverpool’s A& E, during last winter and it didn’t improve much in the summer!
Every MP in Merseyside is Labour and most of those in Cheshire. We do not have to wait for a general election. Our MPs must step up and save lives in the NHS.
What you can do to help us encourage the Government to respond to the threat to life and limb in the current NHS situation?
Talk to family, friends, workmates, fellow students, and neighbours about the need to rescue the NHS. Every great campaign starts with talking about it.
Write to or email your MP.
Ask for an appointment with your MP.
Give out campaign leaflets in your street.
Put up a poster calling for action for the NHS.
Raise the issue of the NHS with your union. Unions helped found the NHS. They can help persuade the government to act and to act urgently.
Join our campaign
Truly we wont know what we have lost until its gone. Fight for it.
Thanks to Maxine Peake one of our better known supporters.
This is a deliberately detailed post. A shorter version is available here
Making a stand for the NHS.
Major changes to the governance of all the hospitals in Liverpool (except Alder Hey Children’s Hospital) have been announced. This sounds quite boring but it is a symptom of a deeper problem, affecting our NHS, locally, regionally and nationally.
It directly affects the future of Liverpool Women’s Hospital.
The NHS has been denied proper funding for more than a decade and has been repeatedly reorganised on different “business” models.
Our NHS hospitals and out-of-hospital services should run as a whole system service, not as competing businesses.
Healthcare provision is a major investment for any country. We say that investment should prioritise the health of the people and the workforce it employs not the quick buck for private companies.
The NHS was set up as a comprehensive public service, not a business opportunity, and for many years the NHS was the best in the world. In recent decades, for ideological reasons, many different pro-business, pro-privatisation models have been introduced at great cost. This coupled with inadequate funding and poor workforce planning has produced today’s multiple health crises.
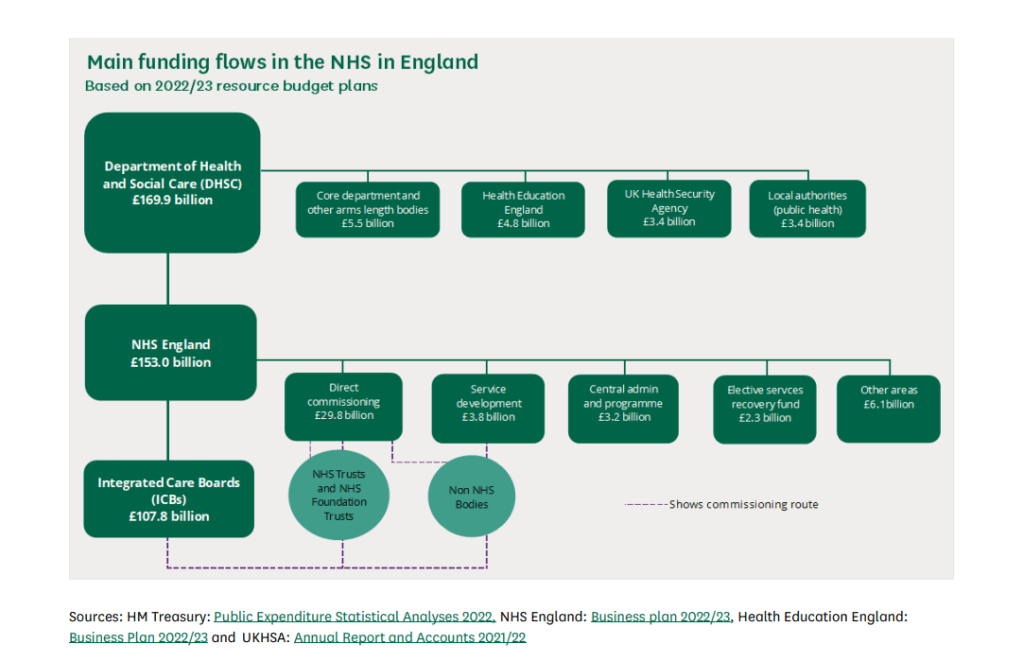
This diagram shows the flow of money into the NHS.
Strands in the NHS organisation structure (as produced by successive pro-privatisation governments).
A. The hospitals and out-of-hospital services like the GPs( primary care).
B. Big businesses including
Those have contracts to run NHS services. There are many private companies operating publicly funded health care for profit. Some of these companies are causing serious system problems for funding and workforce training and problems for patients. There are serious concerns about some of these companies
The political Advisors who advocate the privatisation model to the Government ( Samatha Jone has been removed from the Department of Health.
The forty-two Integrated Care Boards across England
Oversite frameworks like the CQC.
Hospitals and the ICB are in a tug of war for control of the public investment in healthcare. In 2024 the hospitals still function as individual businesses funded by the Government, some have comfortable bank balances, others repeatedly borrow at interest from the Government because they are structurally underfunded. Hospitals with big bank balances are not necessarily providing the best treatment and those having money problems can be providing good services. For more detail see this.
.In 2024 we have the ICB project. which splits the once national health service into 42 organisations modelled on the US ACO system.
This ICB model aims to create a regional organisation encompassing all government-funded healthcare in its region. Managing this crazy situation is National Health Service England (NHSE) and the Government. In our area, Cheshire and Merseyside, the ICB has problems.
“Board members will now be aware that NHS England has assessed the system as being at high risk of not delivering against the system financial plan submitted for the year ahead. Therefore, NHS England has mandated external support to undertake an urgent review. The ICB has engaged Price Waterhouse Cooper as the external support.”
This is not the first time Price Waterhouse Cooper has been called in about Cheshire and Merseyside. Within Cheshire and Merseyside, there are problems specific to Liverpool. These are problems of funding. There are three specialist hospitals in Liverpool that have been centrally funded, something the government intended to change. This is how Carnell Farrar, author of Liverpool Clinical Services Review reported the situation:
“The Cheshire & Merseyside ICS allocation per head to NHS organisations remains higher than all other core cities with the overall allocation due to decrease by c.£three hundred million over the coming years. Alongside this the new Specialised Commissioning allocation will mean that Cheshire and Merseyside will be allocated £50 million less income from specialised commissioning.”
We have seen denial of service, underfunding, the closure of beds and hospitals and the ICB system itself, all causing problems for patients. The work of the health service goes on, though diminished.
Each day a small army of 1.6 million people who make up the NHS staff go to work to provide healthcare and provide the daily miracles of skill, care, and kindness that we expect from our NHS. However, whilst millions are treated, millions of people do not get the care they need and we see many unnecessary deaths and suffering. But the big corporations still make huge profits from our NHS and thirst for more.
The NHS provides treatment for the vast majority of people in the UK though disgracefully, migrants are charged at 150% of the cost, or pay a surcharge for every member of the family, or are denied treatment.The huge scandal of denying treatment to NHS patients rumbles on. But this is what everyone could face if the privatisation project continues. England, Wales and Northern Ireland have slightly different NHS systems but all provide most treatments free at the point of need, funded by the Government.
It’s worth remembering that the US government spends more per person on healthcare, with worse outcomes, and most people pay huge insurance costs on top of Government spending. The US system is dreadful. Yet this is the model the previous government preferred, though it did not dare say so too loudly. Some Other wealthy countries either have a social insurance system or a mix of private and social insurance some use the original NHS model
“Each of the founding principles of the NHS is under attack: a universal, comprehensive service, publicly owned and accountable, funded through taxation and free at the point of use, with decisions on treatment taken on clinical grounds regardless of ability to pay.” (Tony O Sullivan, Keep our NHS Public).
Previous governments, including Labour Governments, have deeply damaged the NHS. What the last government did is qualitatively worse. This video from 2021 by Deborah Harrington from https://publicmatters.org.uk/ is a great description of what we face. What the new government will do remains to be seen, but those who value the work of the NHS must demand full restoration and repair.
Like many other public services, there are deep problems caused by underfunding, various forms of privatisation, and the selling off at knockdown prices of precious public assets. We campaign in the streets for our NHS, liaise with NHS workers, follow the open meetings, organise events and read and share documents. Government sources provide evidence of the situation. This is what the National Audit Office had to say, 23rd July 2024:
“The scale of challenge facing the NHS today and foreseeable in the years ahead is unprecedented.”
‘Deep financial deficits have now spread widely across the NHS and are having a substantial impact on patients. Some NHS trusts have been forced to reduce staffing or delay transformation plans that could give patients faster access and higher quality care when they need it.
The NAO report also says. “As they are statutorily required to do, NHS England and NHS systems have prioritised trying to live within their allocated funding. But, despite great in-year efforts to do so – some of which privilege the short term at the expense of the long term – an increasing number of NHS bodies have been unable to break even.”
The Integrated Care Board, the ICB set up over Cheshire and Merseyside, has financial problems. As a result, a firm called Price Waterhouse Cooper has been brought in to review their spending. Some of this spending is crucial to the safety of Liverpool Women’s Hospital. If Price Waterhouse Cooper disagrees with the ICB, then enforcers can be sent in to make the cuts.
Liverpool has more specialist hospitals than other cities. These hospitals do spectacular work way beyond the city boundaries. They are:
The Clatterbridge Cancer Centre NHS Foundation Trust (CCC), and
The Walton Centre NHS Foundation Trust (TWC).
Specialist hospitals are currently funded nationally, but plans are afoot to bring them into the ICB system. Our specialist hospitals exist because Liverpool is a core city, the largest in its region, surrounded by smaller towns and is a major port. This is not the first time concern has been raised about the future of the specialist hospitals .
Liverpool Women’s Hospital is partially funded by the specialist system, and mostly by the ICB.
Specialist hospitals are funded nationally. In our view, they should continue to be. This allows developments in treatment and expertise.
The new plan
All Liverpool Hospitals, except Alder Hey, will have major decisions made by the Adult Acute and Specialist Hospitals Joint Committee.
“The focus of the joint committee will be to establish the new governance arrangements, meeting in shadow form (i.e. no formal authority) in September 2024 and be in place formally (i.e. with authority to make decisions) by April 2025”.
The Chairs and Chief Executives of the five adult acute and specialist Trusts, outlined below, will sit on the joint committee:
Liverpool University Hospitals NHS Foundation Trust (LUHFT),
Liverpool Women’s NHS Foundation Trust (LWH),
The Clatterbridge Cancer Centre NHS Foundation Trust (CCC), and
The Walton Centre NHS Foundation Trust (TWC).
“This will enable more streamlined decision making and help to build upon existing collaboration with a specific requirement to collectively manage the financial position across the Trusts, deliver economies of scale and manage vacancy controls.” (Our emphasis. So it is about money and jobs).
The plans do not affect Mersey Care Foundation Trust. The proposals were published on the 29th of July. They are a follow-up to the Liverpool Clinical Services Review, produced by Carnall Farrar, one of the financial/business consultants who cost the NHS dear. Full details of the plans can be seen on our previous post.
What is NHS governance? “Governance” is defined by the NHS as
“the means by which provider boards direct and control their organisations so that decision-making is effective, risk is managed and the right outcomes are delivered.”
Trusts are already expected to cooperate with the local Integrated Care Board, the ICB.
“In addition to their existing duties to deliver safe, effective care and effective use of resources, the success of individual NHS trusts and foundation trusts will increasingly be judged against their contribution to the objectives of the ICS.”
The NHS currently operates within several models of organisational privatisation. Trusts were introduced in 1990. They were intended to make hospitals operate like businesses on the United States model. Then in the Health and Social Care (Community Health and Standards) Act 2003, Foundation Trusts were established. Then came the 2012 Act which brought in the commissioning of services to allow private companies to bid for NHS services. This legislation makes Trusts act like competing businesses. Then the 2022 Act brought in the ICBs which split the national NHS into forty-two different self-governing areas, modelled on the US Accountable care systems. The trusts still have legal rights but the ICB currently holds the money and with it the dominant power.
We call for a return to the original public service, not-for-profit-system, the Bevan model. The Bevan model was the most cost-efficient and the most equitable way of running healthcare and made the NHS for many years the best health service in the world. Look at where we are now!
For the patients, ‘system working’ (cooperation rather than competition between hospitals) is better than the ‘business’ model. For privatisers the ‘business’ model is more profitable and, long-term, will produce a system easier for to privatise and manage profitably.
The pandemic forced hospitals to function as a system not as competing entities and it worked! This is when CMAST mentioned above was set up.(See point 2.1 of this)
At the heart of this are the drive to cut NHS spending services, and workforce to make privatisation easier. The following are quotes from the Carnell Farrar report called Liverpool Clinical Services Review. There were fears for the specialist hospitals when the Carnell Farrar Review was published. Quite clearly funding is a key issue.
The misguided proposal to move Liverpool Women’s Hospital to the Royal has, fortunately, been withdrawn, as no funding was available. The idea of moving the Women’s Hospital to the Royal did not even get onto the ill-fated ‘forty new Hospitals’ promised by Boris Johnson.
We would rather the NHS management had focused on patient care and staff wellbeing. Below are direct quotes from the Carnall Farrar report which underline the key importance they give to finance.
1.Currently, NHS organisations in Liverpool are in financial deficit with an aggregated reported deficit position of £12.3 million at YTD (August 2022/23), which is expected to deteriorate further over the rest of the financial year.” (Carnell Farrell Report).
2. The Cheshire & Merseyside ICS allocation per head to NHS organisations remains higher than all other core cities with the overall allocation due to decrease by c.£three hundred million over the coming years. Alongside this the new Specialised Commissioning allocation will mean that Cheshire and Merseyside will be allocated £50 million less income from specialised commissioning. Local government in Liverpool and across Cheshire and Merseyside has also seen one of the largest decreases in real terms spending power since 2010 with a decrease of £700 per head of the population”. (Carnell Farrar Report).
3. “Liverpool has the greatest extent of deprivation in England as measured by the Index of Multiple Deprivation (IMD), with two in three people living in deprivation, and eight in every hundred people living in the most deprived one percent of the country. With respect to income, Liverpool is the most deprived local authority, and the most deprived with respect to employment and living environment.” (Carnell Farrar Report)
We oppose these plans because.
The changes involve Liverpool Women’s Hospital and Liverpool’s Specialist Hospitals which are The Clatterbridge Centre, Liverpool Heart and Chest Hospital, and the Walton Centre. They each provide care beyond the city boundaries. But this decision system will focus on Liverpool.
Liverpool Women’s Hospital works closely with other hospitals not in this network.
Hospitals already collaborate across Cheshire and Merseyside. The Cheshire & Merseyside Acute & Specialist Trusts provider collaborative (CMAST) already exists to coordinate work across all the Acute and Specialist hospitals in Cheshire and Merseyside so cooperation and coordination are working before the proposals.
These plans appear to be designed to restrict spending and we need more spending, more resources.
These plans distance spending decisions from clinical and social necessity and put a greater distance between decision-making and the real life of the medics, hospitals, and patients.
The plans do not include mental health provision, nor the out-of-hospital services provided by Mersey Care NHS Foundation Trust. Yet on Wirral, there is a drive to merge Wirral Community and Healthcare Trust with Arrowe Park Hospital, (Wirral University Teaching Hospital NHS Foundation Trust, WUTH). The plans affect Clatterbridge, who have a hospital on the Wirral working with WUFT and Wirral Community Health and Care Trust.
The way money is allocated is as important as how much is allocated. We know how maternity has been treated in other hospitals
The World Bank says “How service providers are paid matters as much as how much they are paid”.
The further the money planning is away from the doctors, nurses, and midwives, the further it is from patients’ needs.
The plans further the interests of those imposing the ICB system more deeply upon our NHS.
The changes impact Liverpool Women’s Hospital. Liverpool Women’s Hospital serves way beyond Liverpool. It is a tertiary service taking cases across the area and beyond. It is a regional maternal medicine centre. We have a national maternity crisis. As the largest Maternity Hospital the problems with the Maternity tariff and the maternity insurance scheme impact LWH the most.Liverpool Women’s Hospital must focus on providing maternity care and women’s health. It needs cooperation with other hospitals, including but not only LUHFT. It must not have its financial decisions made by the much larger Liverpool University Hospitals Trust nor by the combined committee of the Liverpool Hospitals.
Maternity decisions should be made by people who know most about maternity. After all the reports on maternity problems, how can it now be relegated to a subdivision of a big hospital group?
Liverpool Women’s Hospital needs more midwives, a 24/7 consultant presence, better blood services and diagnostics and a medical team to tackle suddenly deteriorating patients. Above all, it does not need cuts.
However clever these management geeks are (they are not medics), they cannot solve the nationally caused problems faced by Liverpool Hospitals. They cannot turn on the taps for extra resources, but they can shut off vital money. It is gaslighting the city to pretend that new organisational layers can change the situation.
Every supporter of the NHS wants to see money going to front-line services, not to bureaucracy, not to outsourced privatised services. Everyone objects to the waste of money. These proposals do not address those issues. They create yet another layer of bureaucracy and financial control. Financial control often means implementing cuts.
Locally iaison between the hospitals already exists, through CMAST, Cheshire and Merseyside Acute and Specialist Trusts Collaborative, set up to good effect, during the pandemic, despite the privatisation and the business models.
These proposals will not go to public consultation. This is despite a written promise of consultation.
“Patients and public will be involved in the next stage, which is to develop proposals and to strengthen collaboration”.
Save Liverpool Women’s Hospital published these proposals as soon as we saw them. These plans include fundamental changes to Liverpool Women’s Hospital Board of Directors. The board is where long-term decisions are made about the hospital and where the public can catch a glimpse of what is happening. Liverpool Women’s Hospital will experience a two-fold impact, the joint board with LUHFT and the new super layer of management for Liverpool Hospitals.
“Shared Board of Directors for Liverpool University Hospitals NHS Foundation Trust and Liverpool Women’s NHS Foundation Trust”
Our health service is in crisis. It is inadequately funded and inadequately staffed and this situation causes preventable deaths, pain and suffering. For some people, this is death or pain and suffering during pregnancy and birth.
There is a national maternity crisis
This has been the subject of many authoritative reports that the last government failed to address. Another such report is due soon about scandals in Nottingham. Please see our other reports on this scandal. The House of Lords library provided a somewhat restrained summary of reports in January 2023. Maternity Service requires considerable extra funding to be truly safe and well-staffed.
There are unnecessary deaths, pain and suffering because of health service underfunding, understaffing and pro-business reorganisation. There are many millions of patients on long waiting lists for treatments, and crises in Accident and Emergency, mental health, maternity, dentistry and GP services.
The political intention has been to move our publicly funded and publicly provided healthcare to one which serves big business. We can hope Labour changes this, but Streeting is a fan of the private sector. This situation has been decades in the making since Thatcher. In this time fortunes have been made and hospitals have gone short.
The largest Tory Party donor who commented on wanting to shoot Diane Abbott MP, according to the Guardian, made his fortune from privatising services to the NHS.
“Hester, a businessman from West Yorkshire, runs a healthcare technology firm, the Phoenix Partnership (TPP), which has been paid more than £400m by the NHS and other government bodies since 2016, primarily to look after 60m UK medical records. He has profited from £135m of contracts with the Department of Health and Social Care (DHSC) in less than four years.”
No government has been fully open about supporting privatisation but privatise they did. Before any corporation would take over health care the government had to make it fit for profit. Beds and hospitals were closed. Hospital management was moved to an expensive business model, like the foundation trusts, where hospitals were expected to compete like businesses. This way, if a company took over, its responsibilities would be limited to the actual hospital and not the community. In 2015 a company, Circle, took over a major hospital. It was a disaster. It did not work, but the ongoing costs of the “business model” continue today.
A US model, called Accountable Care, (but then renamed in the UK as the Integrated Care System ), was introduced in the 2022 Health and Care Act. The Accountable Care model provides limited health care to the poor whilst giving great profits to the big corporations. You can read about it from the view of those who espouse this system here The focus is clearly on the providers capacity to make money.Many think tanks and commentators espoused the model yet now claim they are horrified at the state of the NHS.
The NHS now has inadequate money, fewer beds, insufficient doctors, nurses and midwives, and workforce planning has been appalling.
When NHS staff sat down to work out how to deliver services with inadequate money and inadequate staff, few if any intended what happened. And what did happen? The appalling planning for COVID, the destruction of mental health services, the damage to the GP service, the maternity crisis, huge waiting lists, and appalling situations in A and E. It is the cumulative effect of years and years of cuts, underfunding, corporate-style reorganisations and sheer wear and tear on the staff.
Why are these plans confined to Liverpool? Why should a Liverpool-only committee make decisions about hospitals with a wider reach? Liverpool has an unusual number of specialist hospitals. They treat people from a wide area because they are specialists. They provide treatment that ordinary hospitals could not afford to fund or research. They are centres of excellence and research for staff. This new layer of management won’t provide extra expertise but it will create a situation where the
“focus of the joint committee will be on the management of capacity and demand, workforce challenges, collective financial management and governance arrangements for the five organisations”
It will also “Tackle challenges including the significant funding gap.”
Can this new committee tackle the workforce challenges for the most specialised fields in medicine? Solve them in one city? It can though restrict funding or divert funding. We say maternity and mental health have had enough of such restrictions already, do not let the other specialist hospitals go the same way.
The government wants (wanted?) everything under the auspices of the ICB. Then they could follow the US model and hand a whole ICB to a big US health corporation to manage for a lump sum. What the corporation does not spend becomes their profit, but that decision is theirs. You know, like the water companies and the railways?
The ICB provides the money. Why should there be another funding control except to restrict services just in Liverpool? Reading all the papers for board meetings for the Trust and for the ICB is challenging enough. Now these five members of this new committee are going to have to be familiar with all the specialist hospital issues, all the Maternity, Neonatal and Women’s health issues and the huge acute hospital and then make financial decisions, but only about Liverpool, although the hospitals deal way outside of the city boundaries.
We do not yet know what improvements in funding the current government will make, but the CEO of the ICB said at the July 2024 meeting that he did not expect significant changes.
Privatisation of public services has been an unmitigated disaster, from the excrement in the rivers and sea to, the utterly unreliable railways, and the neglect of children taken into care. Already there are huge differences in health services in different areas.
LUHFT ( The Royal Broadgreen and Aintree Hospitals) also provides specialist services way beyond Liverpool. For example, we know of people travelling to the St Paul’s Eye Hospital from as far away as Cornwall. The outpatient clinical space provision for St Pauls, before the new building, was frankly dreadful with cramped rooms for eye testing, difficult even for those with good sight to manage. How could a small specialist provision compete in a budgeting competition with immediate life-preservingservices? These proposals would put the Specialist Hospitals in Liverpool under similar budget and organisational pressures to what St Pauls experienced in LUHFT.
There must be an end to cuts. An end to shaping health service systems on failed “business” models.
NHS services must be well-funded and well-staffed, with excellent laboratory backup, ambulance services, and effective care in the community. The fabric of the buildings must be adapted to demand to ensure safe environments for patients and staff. Working conditions, and the employment of fully qualified medical, midwifery and nursing staff as a priority. Workforce planning and staff retention must all be addressed.
Normally when hospitals cannot cope safely with the budget they are allocated, they apply for “drawdowns” from NHSE, England’s top NHS funding body. NHSE is currently refusing to give such monies to some hospitals. The Health Service Journal commented that “trusts are more likely to have their applications rejected or receive less than they asked for. Major trusts have warned of “slippage” in payments to suppliers.
“An email from NHSE’s finance team, seen by HSJ, said trusts applying for support need to provide assurances from their chair and CEO that they are on track with financial plan; have cash and cost controls in place; and confirm their workforce plans are on track.”
“Confirm their workforce plans are on track” does not mean they are to hire the doctors, nurses, and midwives they need, but the opposite. One whole ICB and their trusts have been sanctioned for recruiting too many staff.
We, with other campaigners across Merseyside, Cheshire,Lancashire and nationally, will keep up the fight to restore and repair the NHS. We will be lobbying Labour’s Conference, in Liverpool, in September. Please help by writing to your MP demanding the restoration and repair of the NHS.
Lets use this opportunity to make the case for a return to the Bevan Model of the NHS
More than 70,000 people have signed our petition to Save Liverpool Women’s Hospital online and on paper. The paper petitions represent 20,000 individual conversations about these issues.Please continue your suport.
The Hospitals in Liverpool, and just in Liverpool, under pressure from the ICB, intend to set up a further layer of “governance” to manage finances and drive some greater cooperation. This committee is called the Adult Acute and Specialist Hospitals Joint Committee. The ICB controls all the finances for hospitals across Cheshire and Merseyside.
We like the cooperation idea, but not the idea of both the specialist hospitals and the Women’s Hospital being in unequal competition with the main hospital services for priorities and funding. Liverpool Women’s Hospital already has an imposed shared CEO, Chair, and other officials with Liverpool University Hospitals Foundation Trust (the Royal, Broadgreen and Aintree), all men, people with no published expertise in women’s health or maternity.
These proposals mean that Liverpool Women’s will have a completely shared board with the Royal, Aintree and Broadgreen Hospitals, and have their decisions further scrutinised by this additional board which will also cover the specialist hospitals in Liverpool. These hospitals are.
Liverpool Heart and Chest Hospital NHS Foundation Trust (LHCH),
The Clatterbridge Cancer Centre NHS Foundation Trust (CCC), and
The Walton Centre NHS Foundation Trust (TWC).
How will women and babies fare in this further layer of bureaucracy? How does this fit in the spirit of the Ockendon report? How will the specialist hospital services fare?
These hospitals serve a wide area, not just Liverpool.
We took twenty thousand signatures to the ICB and were promised consultation.
We were promised consultation on any future plans. Those promises are being broken.
The waste in the NHS is in privatisation and the failed “business” model. The original NHS model, the Bevan model is much more cost effective. The big acute hospitals need better funding and staffing as do the specialist hospitals, though it is not just funding that is needed. We want the NHS restored and repaired.
The evidence is clear. We need more midwives and a better maternity service. Patients need access to GPs, an end to huge waiting lists, access to well-functioning Accident and Emergency care and better cancer treatment. We need to be able to get a dentist’s appointment without our bank or credit cards creaking. There are millions of people on waiting lists. GP services are in disarray and GPs are taking protest action. Mental health services are severely damaged. In Cheshire and Merseyside, 75% of young people asking for help with their mental health get nothing. NHS staff need better pay and much better working conditions.
We need all our children to be well fed, for the good of their health and well-being now, and to prevent chronic illnesses in later life. The UK is the worst country for increasing child poverty. Far too many of us in Liverpool are poor or hard up. This can make us forget that we live in a rich country, one that can afford good public services. For decades Liverpool people fought for health care till we won the NHS. We want a return to the original NHS model where hospitals are not competing but cooperating and pursuing their specialisms. We must insist this new Government funds the NHS and restore it to the original Bevan model that less than ten years ago made it the best health service in the world. Funding healthcare is a great investment for a government to make. It is good for people’s health and for the economy.
Speak up for the NHS.
Talk to your neighbours and family about the NHS.
Join our campaign. Sign the petition if you have not already signed.