All NHS services in Cheshire and Merseyside, including Liverpool Women’s Hospital, are affected by cuts made in 2025-2026 by the Integrated Care Board. The financial situation this year, 2026-27, is set to be worse unless the people have a say and persuade the politicians that this is a very bad decision. MPs need to hear from the public on this issue. You can write to them. They work for you.
You can also raise the matter with your union, with your community groups, with families. People need to know, so we can win the case for much better funding and an end to creeping privatisation. This government has u turned before when they realise how unpopular their decisions are.
The major issues of the Maternity Crisis are directly affected by this financial squeeze, as evidenced by the problems described as “capacity pressures” in Baroness Amos’s interim report. We continue to campaign on this.
We wrote in detail about the Cheshire and Merseyside 2025-2026 budget in a post last year. Sadly, our fears were realised.
We are working with other campaigns and unions fighting for the NHS. Please get involved if you can. This is the press statement that NHS campaigns across Cheshire and Merseyside have issued ahead of the Cheshire and Merseyside ICB meeting on 26 03 2026, where the cuts will be discussed in detail. We will update this post or make another post reporting on what happens at this meeting.

Press Statement
From NHS campaigns in Cheshire and Merseyside, including Keep our NHS Public Merseyside, Defend our NHS, Save Liverpool Women’s Hospital, and other groups.
Cheshire and Merseyside 26 03 2026
Campaigners protest the utterly unacceptable funding for the Cheshire and Merseyside NHS.
“Utterly unacceptable: Cheshire and Merseyside NHS is expected to make further service cuts in the 2026-7 budget year. This follows the grave situation in 2025-26. We urge MPs to protect our area and address these proposals, and call on the ICB to consult the public. We call on the public to rally behind our NHS.
Cheshire and Merseyside NHS ICB meets on Thursday 26 March 2026 at The Conference Suite, Riverside Innovation Centre, 1 Castle Drive, Chester, CH1 1SL.
In 2025-26, deep cuts led to corridor care, long wait times, the use of inappropriate wards, and longer delays in planned treatment—impacting even children and Maternity units—and the ICB papers point to another winter crisis next year. Hospitals had to rely on” distressed funding “to pay their routine bills. Cutbacks affected staff recruitment / filling vacancies, with freezes compounding the effect of staff shortages and a target of 15% headcount reductions. This even included cutting cleaning staff, while hospital-acquired infections are at problematic levels. Qualified staff are unable to find work. Reduced rates paid to staff for covering extra shifts means leaving many shifts uncovered. Patients and staff suffered.
Stretching staff ratios has a significant effect on patient outcomes. This was made clear in the Covid enquiry into the NHS, published this week. Decisions on staffing levels are political, and there is widespread concern about these developments.
Several Cheshire and Merseyside hospitals face mandates to cut costs, including the Countess of Chester, the Liverpool Hospital Group, and Wirral University Teaching Hospitals.
This is not a reallocation of funding to out-of-hospital care, which continues to face difficulties. There have been significant redundancies within the ICB while additional duties have been placed on the NHS. The ICB also paid PricewaterhouseCoopers £5 million for efficiency advice while reducing staff who might otherwise have performed similar work.
The focus of the Cheshire and Merseyside NHS Integrated Care Board on Thursday, 26 03 2026, is on reducing spending, as seen in its single improvement plan (page 148). Cheshire and Merseyside NHS is expected to manage further funding reductions. This year’s real-terms budget increase is 0.5%, even as poverty, inadequate housing, food insecurity, and low wages rise, and as an ageing population requires more medical support.
We value our NHS and are grateful for the skill, dedication, kindness, and humour of our NHS workers. Investment in healthcare grows the economy, and these deep cuts threaten the service we depend on and the wider economy, locally and nationally.
Reference articles
https://www.hsj.co.uk/quality-and-performance/mapped-rtt-waiting-times/7041284.article
https://www.cheshireandmerseyside.nhs.uk/get-involved/upcoming-meetings-and-events/nhs-cheshire-and-merseyside-integrated-ca See page 148.
Liverpool Women’s Hospital
Liverpool Women’s Hospital is directly affected by these issues because it is underfunded, and only changes to the national Maternity Tariff will address that. The Maternity tariff is, according to NHS England, “a structured payment system used by commissioners to pay healthcare providers for Maternity services, usually via a ‘Maternity pathway payment’. In the warning letter about not meeting financial targets sent to Liverpool Women’s Hospital, theysaid “3.2 The PricewaterhouseCoopers FY25/26 Rapid Financial Diagnostic carried out across the Cheshire and Merseyside Integrated Care System in June 2025, highlighted the following issues and financial risks at the Licensee: 3.2.1 the National Maternity Tariff does not meet the full cost of Maternity services at the Licensee which include increased patient complexity and acuity which is driving changes in the case mix (for example, growth in deliveries by caesarean section in recent years) and interventions.” so NHSE themselves say the hospital does not get enough money but must continue to make cuts.

The NHS is an essential and much-loved service, but it has been badly damaged. The staff work wonders, actual wonders in many situations, but the workload is becoming unbearable. At the Covid Enquiry, the Chief Medical Officer said, “Running the NHS at almost full capacity in peacetime is a Political choice” Bed occupancy is as high as before Covid. For more information on bed occupancy, this is a good read. That is a political choice and a bad one.
Poor housing, low wages, expensive food, air pollution, and expensive heating all contribute to poor health, but that is no excuse to underfund healthcare, while we have a system that could provide that care. Good healthcare helps grow the economy. Denying children swift access to quality healthcare creates problems for the rest of their lives. How expensive is that?
The ICB receives funding from the National Health Service England and shares it between hospitals and other providers. This money is simply not enough to provide all the required services. Five out of seven local hospital trusts are being warned of “overspending “and not producing sufficient “Cost Improvement Plans”.These trusts include Liverpool University Hospitals NHS Foundation Trust, Liverpool Women’s Foundation Trust, Mid Cheshire Hospitals Foundation Trust, Countess of Chester Hospital Foundation Trust, and Wirral University Teaching Hospital FT. Cheshire and Merseyside ICB had the worst “overspend” in the country – but we need this funding for patient care.
Liverpool University Hospitals NHS Foundation Trust, with the highest “overspend”, serves the most deprived catchment area of any NHS trust in the country.
There were cruel cuts at the ICB level last year to fertility services, celiac services, and even funding for reducing waiting lists for children. At the same time, £5 million was allocated to pay for financial advice from PricewaterhouseCoopers. Each hospital was expected to make more cuts.
This “overspend” is affected by Government decisions to (nationally) “equalise” spending across areas, but this does not account for differing levels of need. The Nuffield Trust commented in 2025
“Regionally, the deepest deficits are in the North West (2.2% of revenues) and the Midlands (1.5% of revenues), which, along with the North East and Yorkshire, have also seen the steepest declines in financial health since 2022/23.
Acute hospital trusts serving the most deprived patients experienced the steepest declines in their finances in the year to 2023-24, while those serving the smallest proportions of deprived patients experienced modest improvements.
This extreme form of accounting is similar to the US Accountable Care system, but the Accountable Care system is based on a private profit model. The NHS is supposed to be a universal public service.
We want value for money and healthcare driven by human need, not human greed.
We do not need the more than £1.8 billion wasted on privatisation and financial consultants, nor do we need the one-billion-dollar pharmaceuticals deal with Trump.
““In a letter to the House of Commons Science Innovation and Technology Committee on 30 January,1 Vallance said the deal—which includes a commitment for the UK to double its spend on branded pharmaceuticals from 0.3% of GDP to 0.6% of GDP by 20352—would cost the NHS an extra £1bn by 2028-29 over the remaining three years of the current spending review.3“
Meanwhile, the situation for patients and staff gets tougher. Vacancies go unfilled, and shifts are not covered. Staff are carrying the burden of the cuts. Patient treatment inevitably suffers from hospitals working above safe bed occupation levels and the increased risk of hospital-acquired infections.
The British Medical Association have issued a statement on 12 03 2026 saying that the cuts are “putting patients at risk”
“Doctors say that NHS England has imposed financial restrictions on Integrated Care Boards (ICB) – the NHS organisations which plan and manage healthcare services in a region – and NHS trusts that are damaging patient care and resulting in unreasonable consequences for staff. As a result of these funding restrictions, the ICB in Cheshire and Mersey have introduced recruitment freezes, plans to reduce staffing levels despite significant workload demands, has imposed limits/bans on agency workers, and has unilaterally reduced overtime rates.
In a BMA survey in the region, 88% of respondents said they believe that funding cuts are seriously harming the delivery of safe patient services. 92% of respondents to the survey support formally entering a trade dispute should the matter not be resolved, and 80% of respondents support industrial action should it be deemed necessary.
Doctors are saying they are “overwhelmed” and that morale amongst staff is at an all-time low, with many left to cover unmanageable patient numbers with staffing cover that does not meet required safe levels.
The NHS has fewer hospital beds and staff than other wealthy European countries, which often have far lower levels of poverty. Poverty makes people more likely to get ill, to have multiple pr health issues and to die younger.
Our elders are suffering badly when they go to the hospital via the Accident and Emergency system.
“Shocking new analysis by Age UK in 2024/25 shows there were more than 100,000 instances of over-65s waiting between one day (24hrs) and three days (72hrs) in A&E after a decision to admit them had been made. In more than half (54,000) of these cases, these older people were aged 80 plus.Data reveals “exponential increase in the last 6 years – in 2018/19, people aged 65 plus experienced a wait of between one and three days in A&E only 1,346 times.”
Our area is one of the worst hit by poverty, especially amongst children. In some Liverpool wards, two out of three children live in poverty.
“The child death rate for children resident in the most deprived neighbourhoods of England was more than twice that of children resident in the least deprived neighbourhoods.“
Staff are working as hard as ever, yet the problems remain unresolved. More than 3 million people are waiting for treatment. The winter crisis will (according to Wes Streeting) continue next year or even until the general election. Long waiting lists will continue, although some patients have been removed from the list. Well-qualified staff are unable to get employment. The poorest areas get the worst GP funding, but GPs are unemployed or working outside of medicine. The new GP funding structure is not popular with GPs.
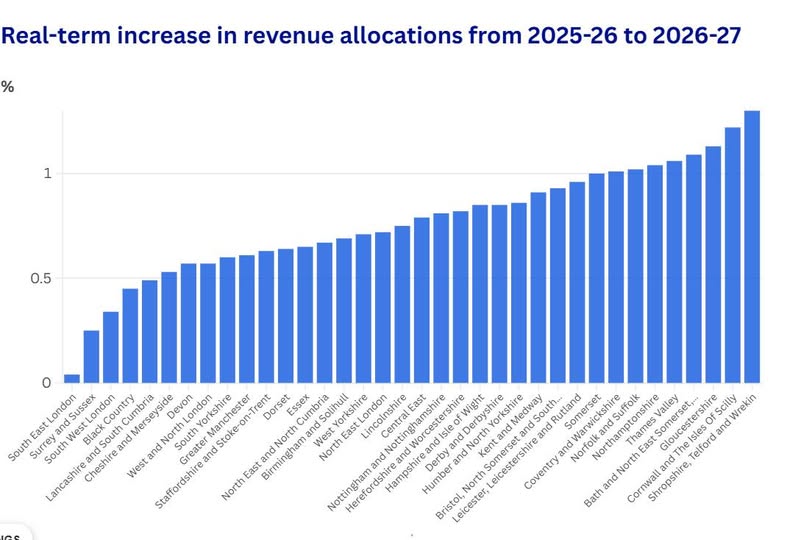
The budget for 2026-27 will be even worse. This article from the Health Service Journal spells out how our area will be one of the worst hit.
No to Palantir
Palantir is a secretive US spy-tech company tied to Donald Trump, with a terrible track record worldwide. It runs the NHS “federated data platform”. We can’t trust them with our health data, and we can’t trust them to respect the values of our NHS. The BMA warns that the Palantir partnership “threatens to undermine public trust in NHS data systems” and highlighted a “lack of transparency in how the data will be stored and processed”. https://notopalantir.goodlawproject.org/
We say.
Restore the NHS
as a publicly-owned, publicly-delivered public service. Privatisation is expensive and damaging to patient care and to the cooperative working of the healthcare system. Restore the funding that used to be directed at areas of poverty. Restore the public service funding model. Remove the “market” model. Restore staff working conditions.
NHS staff have increased workloads, unfilled vacancies, and pathetic pay rises, with pay still not matching the 2014 level in real terms.
Repair the NHS.
Where buildings and equipment are in a poor state, they should be repaired. Repair services where the quality of care has deteriorated. Bring all mental health back into the NHS. Make the NHS once again a good place to work and get care.
Rebuild the NHS.
Where services have been cut, they should be reinstated. Mental health dentistry and Maternity are badly hit.
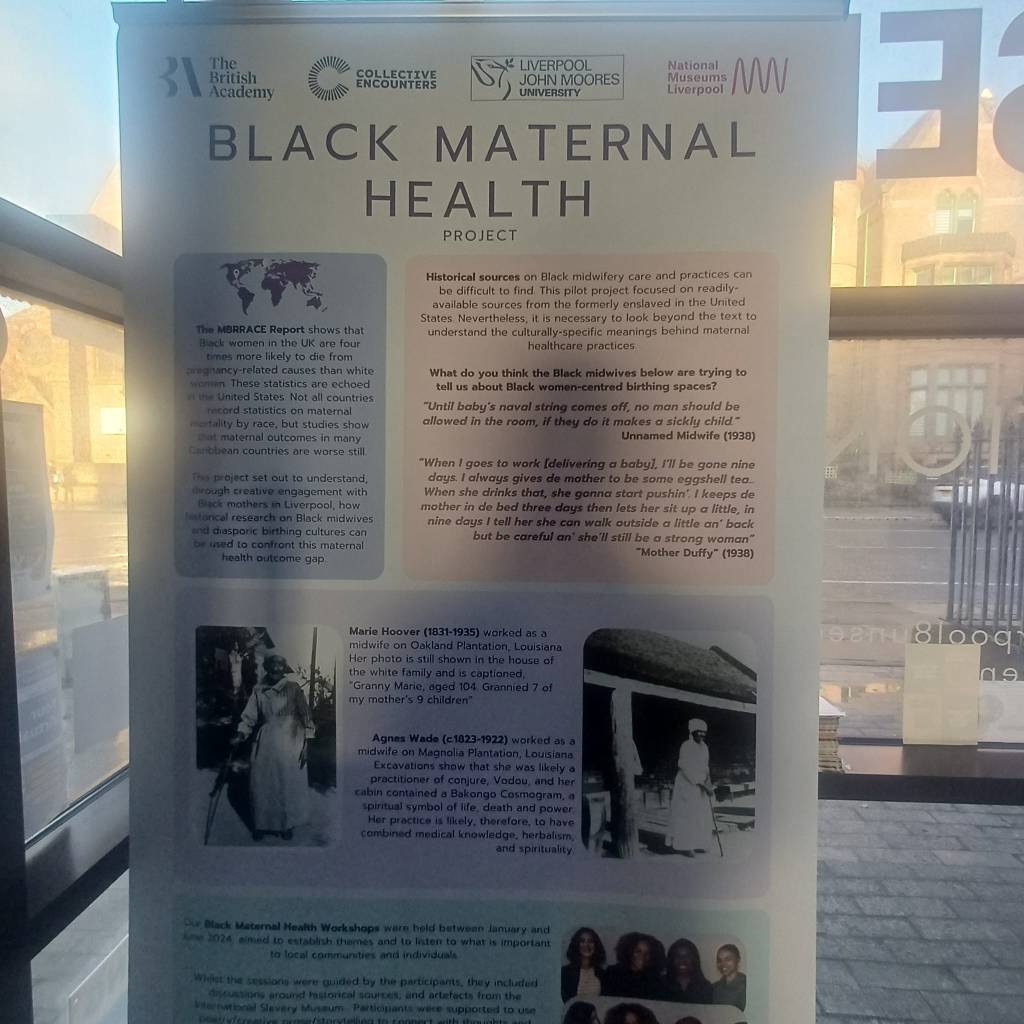
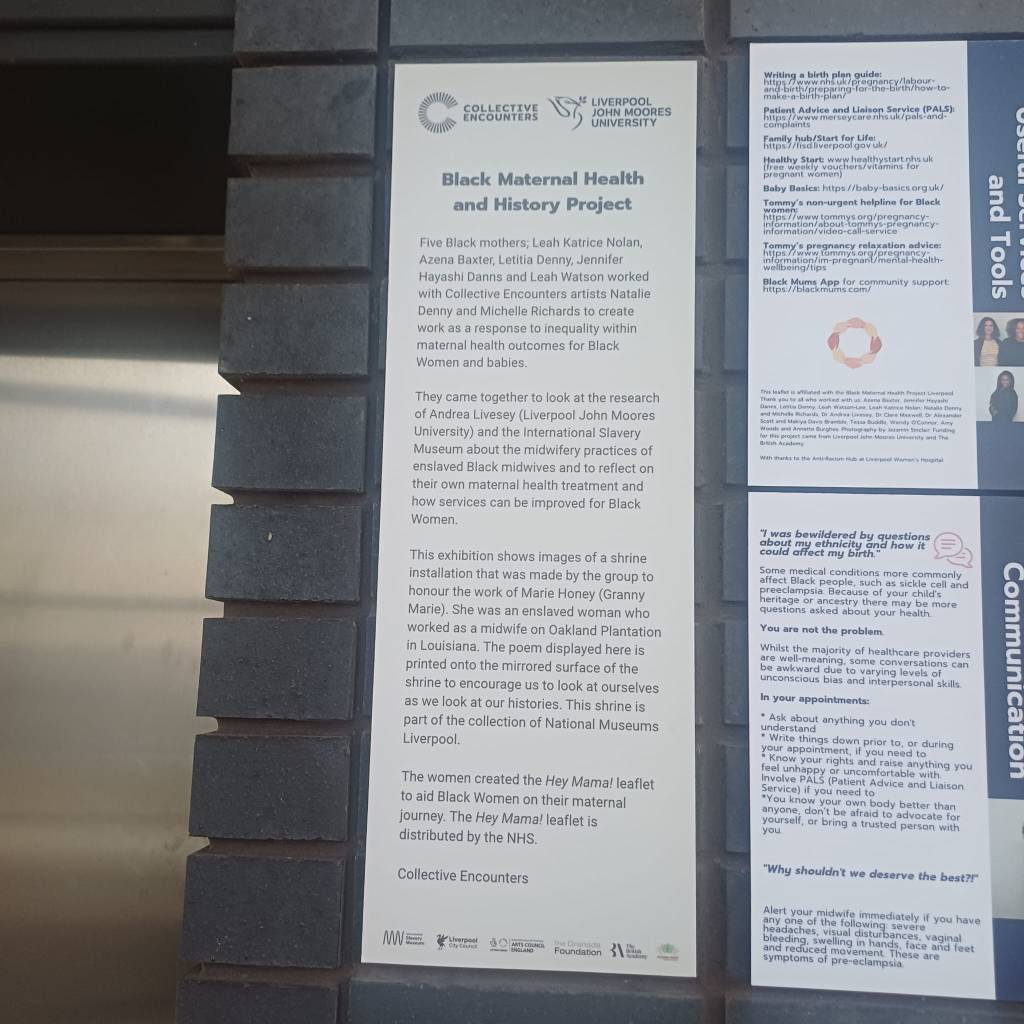
Maternity Crisis: The government can and must invest in NHS finance and staffing for the Maternity service, locally and nationally. Save Liverpool Women’s Hospital. Ormskirk Maternity is also now facing closure. Join the fight for Maternity, women’s health and the whole NHS
This requires investment. We remind politicians that health care expenditure that reaches patients, staff and resources is an investment that gives great returns. We will not suffer in silence
What you can do
• Talk about it with friends,
• Raise the matter at work and in your union branches.
• Put leaflets through doors. Put posters up in shops.
• Set up local community meetings.
• Write to or email your MPs and councillors. Find addresses on “They work for you” on the internet