We do not accept that our children should go hungry and that our elders must suffer from the cold this winter. Both are wrong and both policies will increase pressure on the NHS.
Our NHS is a matter of life and death, (and the working class die first).
Good healthcare makes a country healthier and wealthier. No country can thrive with poor healthcare. No country should have millions unable to work due to a lack of health care.
Healthcare is a human right. The generation that defeated fascism gifted to us, their descendants, the best system of healthcare in the world. This was according to the US Commonwealth Fund. We are now ranked 10 out of 11. We want our inheritance back. No ifs no buts.
The NHS has been bled dry by privatisation, by bringing in the market into healthcare, by austerity and cuts to real term funding, by appalling workforce planning, by letting maternity as a service decline, by the frightening damage to our mental health service, by cuts to beds and inadequate staffing and by the neglect of the fabric of our NHS buildings. These have all caused grave harm some of which the Darzi report mentions.
But each problem can be reversed by government policy if they so choose. These were policies of the Conservatives. They must not be the policy for Labour too.
Professor Danny Dorling has just exposed the cruel cost of austerity to our children. Our children have been hurt more than any other nation by years of austerity. They are becoming smaller in size,bringing back stories of how in world war one too many men were too small,too stunted in size, by poverty to fight. There must be a full break from this to allow our children to thrive.
Our NHS staff work hard and with great skill, kindness and talent but they cannot cope with this imposed poverty of resources, disorganisation and crumbling buildings.
Mothers are describing traumatic birthing experiences in numbers to big too ignore.Midwives report the problems in the labour wards and in ante-natal and post-natal care. We don’t need to repeat the evidence already given in numerous reports, from respected organisations.
Mr Starmer ( a Labour prime Minister) is refusing to respond to the emergency on our doorsteps this winter until a set of “reforms” are introduced.
Mr Starmer says his priorities are digitisation, ( Lots of money there for the big tech companies but we need midwives.) moving care out of hospitals and producing a healthier population.
We urgently need a publicly owned, not for profit, user designed social care system.That will take huge political will and investment but would make so many lives better. Is this too much for us Mr Starmer?
The government must choose to invest now to achieve vital short-term and long-term goals in our healthcare. They must also design our health care as a public service, not a pig’s trough for the rich to root in for tasty morsels. Governments spent five times the cost of the NHS on Quantitative Easing, they spent billions on the Bankers’ crisis, and they are spending billions on the war in Ukraine. See this article for more on Government spending. The NHS too is a crisis that the government must tackle The last government got hammered in the General Election for its policies. Following the same policies will get the same response.
There must be urgent action.
What are we supposed to do in the meantime? Die quietly? Suffer silently? Sit in pain, and get worse for hour upon hour in A and E? Should we be silent while staff are underpaid and overworked? We need action now before this winter’s crisis kills more of us.
We need action on maternity. Mothers in labour cannot wait. We know all we need to know about how bad the situation is. The reports are numerous. Women and babies need action now.
The GP service is badly damaged and the GPs need a positive response from this government now. All private companies running GP surgeries should be removed. Every available GP should be employed.
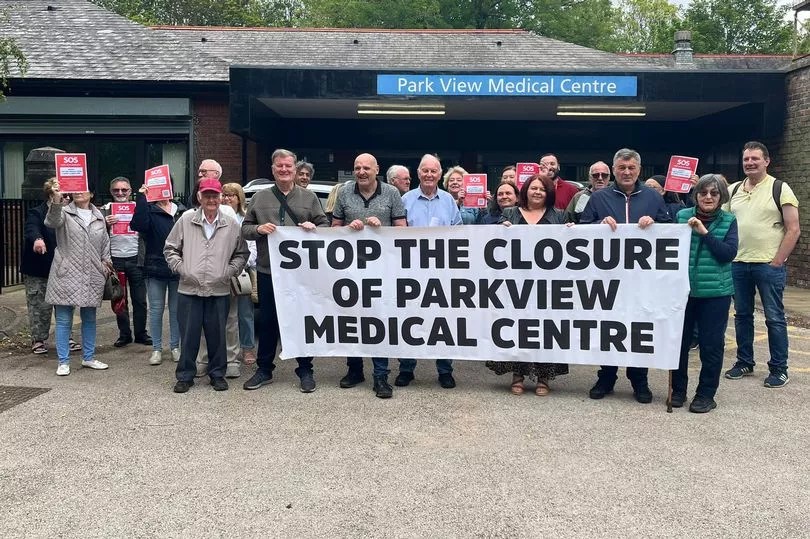
Park View patients protesting the closure of their GP Practice
Patients live longer with consistent access to a GP. The appalling statistics for life expectancy, an life expectancy in good health in poorer areas of Britain make this especially important. In Liverpool the gap in life expectancy between richer and poorer areas is large and the “rich” areas of Liverpool are far from the richest in the country “Life expectancy at birth in Liverpool, is 76 years, although this masks variation, with an average of 76.4 years in Anfield and Everton compared to 83.1 years in Childwall and Wavertree.”The Office for National Statistics said
In 2018 to 2020, male healthy life expectancy (HLE) at birth in the most deprived areas was 52.3 years, compared with 70.5 years in the least deprived areas. Female HLE at birth in the most deprived areas was 51.9 years, almost 20 years fewer than those living in the least deprived areas (70.7 years).
Mersey Pensioners protesting about Physician associates being used instead of fully qualified doctors.
We say
Fund and organise action now to improve the situation for this coming winter, including lifting financial restrictions, opening more beds recruiting staff, make more space available.
Improve maternity funding immediately so hospital managers are not pushing staff to cope with too few resources, and too few staff. Improve the maternity tariff. Improve the ratios of midwives to birthing mothers. Bring back health visitors. Tackle infant mortality. Try to win back some of the staff who have left in disgust at the poor state of maternity. Heed what women are telling you about maternity. Stop the epidemic of birth trauma
Save Liverpool Women’s Hospital, the largest in the UK. No to mergers.
Employ more GPs not less qualified substitutes. Kick US corporations out of our GP practices.
Let’s get back to a national, publicly provided health care, for all, free at the point of need. The poison of privatisation, outsourcing, insidiously introduced charging and the business model has done great harm.
Our health records are and must be private. We know there is huge value and potential profit in the data to be obtained from a large and well-established national health service but that wealth belongs to the people, including the poorest of us. Use only an NHS digitalisation system agreed with doctors and nurses. No external system owned by dubious US corporations should be allowed near the NHS. We saw what Fujitsu did to the sub-postmasters.
You can help.
Photo from the Liverpool Echo of Liverpool’s A& E, during last winter and it didn’t improve much in the summer!
Every MP in Merseyside is Labour and most of those in Cheshire. We do not have to wait for a general election. Our MPs must step up and save lives in the NHS.
What you can do to help us encourage the Government to respond to the threat to life and limb in the current NHS situation?
Talk to family, friends, workmates, fellow students, and neighbours about the need to rescue the NHS. Every great campaign starts with talking about it.
Write to or email your MP.
Ask for an appointment with your MP.
Give out campaign leaflets in your street.
Put up a poster calling for action for the NHS.
Raise the issue of the NHS with your union. Unions helped found the NHS. They can help persuade the government to act and to act urgently.
Join our campaign
Truly we wont know what we have lost until its gone. Fight for it.
Thanks to Maxine Peake one of our better known supporters.
This is a deliberately detailed post. A shorter version is available here
Making a stand for the NHS.
Major changes to the governance of all the hospitals in Liverpool (except Alder Hey Children’s Hospital) have been announced. This sounds quite boring but it is a symptom of a deeper problem, affecting our NHS, locally, regionally and nationally.
It directly affects the future of Liverpool Women’s Hospital.
The NHS has been denied proper funding for more than a decade and has been repeatedly reorganised on different “business” models.
Our NHS hospitals and out-of-hospital services should run as a whole system service, not as competing businesses.
Healthcare provision is a major investment for any country. We say that investment should prioritise the health of the people and the workforce it employs not the quick buck for private companies.
The NHS was set up as a comprehensive public service, not a business opportunity, and for many years the NHS was the best in the world. In recent decades, for ideological reasons, many different pro-business, pro-privatisation models have been introduced at great cost. This coupled with inadequate funding and poor workforce planning has produced today’s multiple health crises.
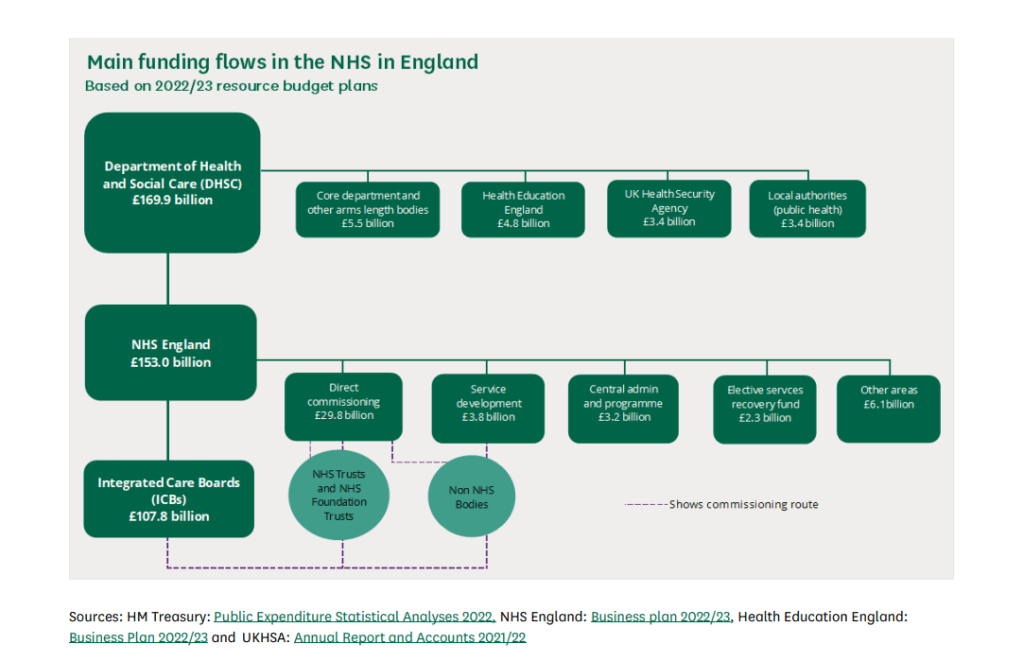
This diagram shows the flow of money into the NHS.
Strands in the NHS organisation structure (as produced by successive pro-privatisation governments).
A. The hospitals and out-of-hospital services like the GPs( primary care).
B. Big businesses including
Those have contracts to run NHS services. There are many private companies operating publicly funded health care for profit. Some of these companies are causing serious system problems for funding and workforce training and problems for patients. There are serious concerns about some of these companies
The political Advisors who advocate the privatisation model to the Government ( Samatha Jone has been removed from the Department of Health.
The forty-two Integrated Care Boards across England
Oversite frameworks like the CQC.
Hospitals and the ICB are in a tug of war for control of the public investment in healthcare. In 2024 the hospitals still function as individual businesses funded by the Government, some have comfortable bank balances, others repeatedly borrow at interest from the Government because they are structurally underfunded. Hospitals with big bank balances are not necessarily providing the best treatment and those having money problems can be providing good services. For more detail see this.
.In 2024 we have the ICB project. which splits the once national health service into 42 organisations modelled on the US ACO system.
This ICB model aims to create a regional organisation encompassing all government-funded healthcare in its region. Managing this crazy situation is National Health Service England (NHSE) and the Government. In our area, Cheshire and Merseyside, the ICB has problems.
“Board members will now be aware that NHS England has assessed the system as being at high risk of not delivering against the system financial plan submitted for the year ahead. Therefore, NHS England has mandated external support to undertake an urgent review. The ICB has engaged Price Waterhouse Cooper as the external support.”
This is not the first time Price Waterhouse Cooper has been called in about Cheshire and Merseyside. Within Cheshire and Merseyside, there are problems specific to Liverpool. These are problems of funding. There are three specialist hospitals in Liverpool that have been centrally funded, something the government intended to change. This is how Carnell Farrar, author of Liverpool Clinical Services Review reported the situation:
“The Cheshire & Merseyside ICS allocation per head to NHS organisations remains higher than all other core cities with the overall allocation due to decrease by c.£three hundred million over the coming years. Alongside this the new Specialised Commissioning allocation will mean that Cheshire and Merseyside will be allocated £50 million less income from specialised commissioning.”
We have seen denial of service, underfunding, the closure of beds and hospitals and the ICB system itself, all causing problems for patients. The work of the health service goes on, though diminished.
Each day a small army of 1.6 million people who make up the NHS staff go to work to provide healthcare and provide the daily miracles of skill, care, and kindness that we expect from our NHS. However, whilst millions are treated, millions of people do not get the care they need and we see many unnecessary deaths and suffering. But the big corporations still make huge profits from our NHS and thirst for more.
The NHS provides treatment for the vast majority of people in the UK though disgracefully, migrants are charged at 150% of the cost, or pay a surcharge for every member of the family, or are denied treatment.The huge scandal of denying treatment to NHS patients rumbles on. But this is what everyone could face if the privatisation project continues. England, Wales and Northern Ireland have slightly different NHS systems but all provide most treatments free at the point of need, funded by the Government.
It’s worth remembering that the US government spends more per person on healthcare, with worse outcomes, and most people pay huge insurance costs on top of Government spending. The US system is dreadful. Yet this is the model the previous government preferred, though it did not dare say so too loudly. Some Other wealthy countries either have a social insurance system or a mix of private and social insurance some use the original NHS model
“Each of the founding principles of the NHS is under attack: a universal, comprehensive service, publicly owned and accountable, funded through taxation and free at the point of use, with decisions on treatment taken on clinical grounds regardless of ability to pay.” (Tony O Sullivan, Keep our NHS Public).
Previous governments, including Labour Governments, have deeply damaged the NHS. What the last government did is qualitatively worse. This video from 2021 by Deborah Harrington from https://publicmatters.org.uk/ is a great description of what we face. What the new government will do remains to be seen, but those who value the work of the NHS must demand full restoration and repair.
Like many other public services, there are deep problems caused by underfunding, various forms of privatisation, and the selling off at knockdown prices of precious public assets. We campaign in the streets for our NHS, liaise with NHS workers, follow the open meetings, organise events and read and share documents. Government sources provide evidence of the situation. This is what the National Audit Office had to say, 23rd July 2024:
“The scale of challenge facing the NHS today and foreseeable in the years ahead is unprecedented.”
‘Deep financial deficits have now spread widely across the NHS and are having a substantial impact on patients. Some NHS trusts have been forced to reduce staffing or delay transformation plans that could give patients faster access and higher quality care when they need it.
The NAO report also says. “As they are statutorily required to do, NHS England and NHS systems have prioritised trying to live within their allocated funding. But, despite great in-year efforts to do so – some of which privilege the short term at the expense of the long term – an increasing number of NHS bodies have been unable to break even.”
The Integrated Care Board, the ICB set up over Cheshire and Merseyside, has financial problems. As a result, a firm called Price Waterhouse Cooper has been brought in to review their spending. Some of this spending is crucial to the safety of Liverpool Women’s Hospital. If Price Waterhouse Cooper disagrees with the ICB, then enforcers can be sent in to make the cuts.
Liverpool has more specialist hospitals than other cities. These hospitals do spectacular work way beyond the city boundaries. They are:
The Clatterbridge Cancer Centre NHS Foundation Trust (CCC), and
The Walton Centre NHS Foundation Trust (TWC).
Specialist hospitals are currently funded nationally, but plans are afoot to bring them into the ICB system. Our specialist hospitals exist because Liverpool is a core city, the largest in its region, surrounded by smaller towns and is a major port. This is not the first time concern has been raised about the future of the specialist hospitals .
Liverpool Women’s Hospital is partially funded by the specialist system, and mostly by the ICB.
Specialist hospitals are funded nationally. In our view, they should continue to be. This allows developments in treatment and expertise.
The new plan
All Liverpool Hospitals, except Alder Hey, will have major decisions made by the Adult Acute and Specialist Hospitals Joint Committee.
“The focus of the joint committee will be to establish the new governance arrangements, meeting in shadow form (i.e. no formal authority) in September 2024 and be in place formally (i.e. with authority to make decisions) by April 2025”.
The Chairs and Chief Executives of the five adult acute and specialist Trusts, outlined below, will sit on the joint committee:
Liverpool University Hospitals NHS Foundation Trust (LUHFT),
Liverpool Women’s NHS Foundation Trust (LWH),
The Clatterbridge Cancer Centre NHS Foundation Trust (CCC), and
The Walton Centre NHS Foundation Trust (TWC).
“This will enable more streamlined decision making and help to build upon existing collaboration with a specific requirement to collectively manage the financial position across the Trusts, deliver economies of scale and manage vacancy controls.” (Our emphasis. So it is about money and jobs).
The plans do not affect Mersey Care Foundation Trust. The proposals were published on the 29th of July. They are a follow-up to the Liverpool Clinical Services Review, produced by Carnall Farrar, one of the financial/business consultants who cost the NHS dear. Full details of the plans can be seen on our previous post.
What is NHS governance? “Governance” is defined by the NHS as
“the means by which provider boards direct and control their organisations so that decision-making is effective, risk is managed and the right outcomes are delivered.”
Trusts are already expected to cooperate with the local Integrated Care Board, the ICB.
“In addition to their existing duties to deliver safe, effective care and effective use of resources, the success of individual NHS trusts and foundation trusts will increasingly be judged against their contribution to the objectives of the ICS.”
The NHS currently operates within several models of organisational privatisation. Trusts were introduced in 1990. They were intended to make hospitals operate like businesses on the United States model. Then in the Health and Social Care (Community Health and Standards) Act 2003, Foundation Trusts were established. Then came the 2012 Act which brought in the commissioning of services to allow private companies to bid for NHS services. This legislation makes Trusts act like competing businesses. Then the 2022 Act brought in the ICBs which split the national NHS into forty-two different self-governing areas, modelled on the US Accountable care systems. The trusts still have legal rights but the ICB currently holds the money and with it the dominant power.
We call for a return to the original public service, not-for-profit-system, the Bevan model. The Bevan model was the most cost-efficient and the most equitable way of running healthcare and made the NHS for many years the best health service in the world. Look at where we are now!
For the patients, ‘system working’ (cooperation rather than competition between hospitals) is better than the ‘business’ model. For privatisers the ‘business’ model is more profitable and, long-term, will produce a system easier for to privatise and manage profitably.
The pandemic forced hospitals to function as a system not as competing entities and it worked! This is when CMAST mentioned above was set up.(See point 2.1 of this)
At the heart of this are the drive to cut NHS spending services, and workforce to make privatisation easier. The following are quotes from the Carnell Farrar report called Liverpool Clinical Services Review. There were fears for the specialist hospitals when the Carnell Farrar Review was published. Quite clearly funding is a key issue.
The misguided proposal to move Liverpool Women’s Hospital to the Royal has, fortunately, been withdrawn, as no funding was available. The idea of moving the Women’s Hospital to the Royal did not even get onto the ill-fated ‘forty new Hospitals’ promised by Boris Johnson.
We would rather the NHS management had focused on patient care and staff wellbeing. Below are direct quotes from the Carnall Farrar report which underline the key importance they give to finance.
1.Currently, NHS organisations in Liverpool are in financial deficit with an aggregated reported deficit position of £12.3 million at YTD (August 2022/23), which is expected to deteriorate further over the rest of the financial year.” (Carnell Farrell Report).
2. The Cheshire & Merseyside ICS allocation per head to NHS organisations remains higher than all other core cities with the overall allocation due to decrease by c.£three hundred million over the coming years. Alongside this the new Specialised Commissioning allocation will mean that Cheshire and Merseyside will be allocated £50 million less income from specialised commissioning. Local government in Liverpool and across Cheshire and Merseyside has also seen one of the largest decreases in real terms spending power since 2010 with a decrease of £700 per head of the population”. (Carnell Farrar Report).
3. “Liverpool has the greatest extent of deprivation in England as measured by the Index of Multiple Deprivation (IMD), with two in three people living in deprivation, and eight in every hundred people living in the most deprived one percent of the country. With respect to income, Liverpool is the most deprived local authority, and the most deprived with respect to employment and living environment.” (Carnell Farrar Report)
We oppose these plans because.
The changes involve Liverpool Women’s Hospital and Liverpool’s Specialist Hospitals which are The Clatterbridge Centre, Liverpool Heart and Chest Hospital, and the Walton Centre. They each provide care beyond the city boundaries. But this decision system will focus on Liverpool.
Liverpool Women’s Hospital works closely with other hospitals not in this network.
Hospitals already collaborate across Cheshire and Merseyside. The Cheshire & Merseyside Acute & Specialist Trusts provider collaborative (CMAST) already exists to coordinate work across all the Acute and Specialist hospitals in Cheshire and Merseyside so cooperation and coordination are working before the proposals.
These plans appear to be designed to restrict spending and we need more spending, more resources.
These plans distance spending decisions from clinical and social necessity and put a greater distance between decision-making and the real life of the medics, hospitals, and patients.
The plans do not include mental health provision, nor the out-of-hospital services provided by Mersey Care NHS Foundation Trust. Yet on Wirral, there is a drive to merge Wirral Community and Healthcare Trust with Arrowe Park Hospital, (Wirral University Teaching Hospital NHS Foundation Trust, WUTH). The plans affect Clatterbridge, who have a hospital on the Wirral working with WUFT and Wirral Community Health and Care Trust.
The way money is allocated is as important as how much is allocated. We know how maternity has been treated in other hospitals
The World Bank says “How service providers are paid matters as much as how much they are paid”.
The further the money planning is away from the doctors, nurses, and midwives, the further it is from patients’ needs.
The plans further the interests of those imposing the ICB system more deeply upon our NHS.
The changes impact Liverpool Women’s Hospital. Liverpool Women’s Hospital serves way beyond Liverpool. It is a tertiary service taking cases across the area and beyond. It is a regional maternal medicine centre. We have a national maternity crisis. As the largest Maternity Hospital the problems with the Maternity tariff and the maternity insurance scheme impact LWH the most.Liverpool Women’s Hospital must focus on providing maternity care and women’s health. It needs cooperation with other hospitals, including but not only LUHFT. It must not have its financial decisions made by the much larger Liverpool University Hospitals Trust nor by the combined committee of the Liverpool Hospitals.
Maternity decisions should be made by people who know most about maternity. After all the reports on maternity problems, how can it now be relegated to a subdivision of a big hospital group?
Liverpool Women’s Hospital needs more midwives, a 24/7 consultant presence, better blood services and diagnostics and a medical team to tackle suddenly deteriorating patients. Above all, it does not need cuts.
However clever these management geeks are (they are not medics), they cannot solve the nationally caused problems faced by Liverpool Hospitals. They cannot turn on the taps for extra resources, but they can shut off vital money. It is gaslighting the city to pretend that new organisational layers can change the situation.
Every supporter of the NHS wants to see money going to front-line services, not to bureaucracy, not to outsourced privatised services. Everyone objects to the waste of money. These proposals do not address those issues. They create yet another layer of bureaucracy and financial control. Financial control often means implementing cuts.
Locally iaison between the hospitals already exists, through CMAST, Cheshire and Merseyside Acute and Specialist Trusts Collaborative, set up to good effect, during the pandemic, despite the privatisation and the business models.
These proposals will not go to public consultation. This is despite a written promise of consultation.
“Patients and public will be involved in the next stage, which is to develop proposals and to strengthen collaboration”.
Save Liverpool Women’s Hospital published these proposals as soon as we saw them. These plans include fundamental changes to Liverpool Women’s Hospital Board of Directors. The board is where long-term decisions are made about the hospital and where the public can catch a glimpse of what is happening. Liverpool Women’s Hospital will experience a two-fold impact, the joint board with LUHFT and the new super layer of management for Liverpool Hospitals.
“Shared Board of Directors for Liverpool University Hospitals NHS Foundation Trust and Liverpool Women’s NHS Foundation Trust”
Our health service is in crisis. It is inadequately funded and inadequately staffed and this situation causes preventable deaths, pain and suffering. For some people, this is death or pain and suffering during pregnancy and birth.
There is a national maternity crisis
This has been the subject of many authoritative reports that the last government failed to address. Another such report is due soon about scandals in Nottingham. Please see our other reports on this scandal. The House of Lords library provided a somewhat restrained summary of reports in January 2023. Maternity Service requires considerable extra funding to be truly safe and well-staffed.
There are unnecessary deaths, pain and suffering because of health service underfunding, understaffing and pro-business reorganisation. There are many millions of patients on long waiting lists for treatments, and crises in Accident and Emergency, mental health, maternity, dentistry and GP services.
The political intention has been to move our publicly funded and publicly provided healthcare to one which serves big business. We can hope Labour changes this, but Streeting is a fan of the private sector. This situation has been decades in the making since Thatcher. In this time fortunes have been made and hospitals have gone short.
The largest Tory Party donor who commented on wanting to shoot Diane Abbott MP, according to the Guardian, made his fortune from privatising services to the NHS.
“Hester, a businessman from West Yorkshire, runs a healthcare technology firm, the Phoenix Partnership (TPP), which has been paid more than £400m by the NHS and other government bodies since 2016, primarily to look after 60m UK medical records. He has profited from £135m of contracts with the Department of Health and Social Care (DHSC) in less than four years.”
No government has been fully open about supporting privatisation but privatise they did. Before any corporation would take over health care the government had to make it fit for profit. Beds and hospitals were closed. Hospital management was moved to an expensive business model, like the foundation trusts, where hospitals were expected to compete like businesses. This way, if a company took over, its responsibilities would be limited to the actual hospital and not the community. In 2015 a company, Circle, took over a major hospital. It was a disaster. It did not work, but the ongoing costs of the “business model” continue today.
A US model, called Accountable Care, (but then renamed in the UK as the Integrated Care System ), was introduced in the 2022 Health and Care Act. The Accountable Care model provides limited health care to the poor whilst giving great profits to the big corporations. You can read about it from the view of those who espouse this system here The focus is clearly on the providers capacity to make money.Many think tanks and commentators espoused the model yet now claim they are horrified at the state of the NHS.
The NHS now has inadequate money, fewer beds, insufficient doctors, nurses and midwives, and workforce planning has been appalling.
When NHS staff sat down to work out how to deliver services with inadequate money and inadequate staff, few if any intended what happened. And what did happen? The appalling planning for COVID, the destruction of mental health services, the damage to the GP service, the maternity crisis, huge waiting lists, and appalling situations in A and E. It is the cumulative effect of years and years of cuts, underfunding, corporate-style reorganisations and sheer wear and tear on the staff.
Why are these plans confined to Liverpool? Why should a Liverpool-only committee make decisions about hospitals with a wider reach? Liverpool has an unusual number of specialist hospitals. They treat people from a wide area because they are specialists. They provide treatment that ordinary hospitals could not afford to fund or research. They are centres of excellence and research for staff. This new layer of management won’t provide extra expertise but it will create a situation where the
“focus of the joint committee will be on the management of capacity and demand, workforce challenges, collective financial management and governance arrangements for the five organisations”
It will also “Tackle challenges including the significant funding gap.”
Can this new committee tackle the workforce challenges for the most specialised fields in medicine? Solve them in one city? It can though restrict funding or divert funding. We say maternity and mental health have had enough of such restrictions already, do not let the other specialist hospitals go the same way.
The government wants (wanted?) everything under the auspices of the ICB. Then they could follow the US model and hand a whole ICB to a big US health corporation to manage for a lump sum. What the corporation does not spend becomes their profit, but that decision is theirs. You know, like the water companies and the railways?
The ICB provides the money. Why should there be another funding control except to restrict services just in Liverpool? Reading all the papers for board meetings for the Trust and for the ICB is challenging enough. Now these five members of this new committee are going to have to be familiar with all the specialist hospital issues, all the Maternity, Neonatal and Women’s health issues and the huge acute hospital and then make financial decisions, but only about Liverpool, although the hospitals deal way outside of the city boundaries.
We do not yet know what improvements in funding the current government will make, but the CEO of the ICB said at the July 2024 meeting that he did not expect significant changes.
Privatisation of public services has been an unmitigated disaster, from the excrement in the rivers and sea to, the utterly unreliable railways, and the neglect of children taken into care. Already there are huge differences in health services in different areas.
LUHFT ( The Royal Broadgreen and Aintree Hospitals) also provides specialist services way beyond Liverpool. For example, we know of people travelling to the St Paul’s Eye Hospital from as far away as Cornwall. The outpatient clinical space provision for St Pauls, before the new building, was frankly dreadful with cramped rooms for eye testing, difficult even for those with good sight to manage. How could a small specialist provision compete in a budgeting competition with immediate life-preservingservices? These proposals would put the Specialist Hospitals in Liverpool under similar budget and organisational pressures to what St Pauls experienced in LUHFT.
There must be an end to cuts. An end to shaping health service systems on failed “business” models.
NHS services must be well-funded and well-staffed, with excellent laboratory backup, ambulance services, and effective care in the community. The fabric of the buildings must be adapted to demand to ensure safe environments for patients and staff. Working conditions, and the employment of fully qualified medical, midwifery and nursing staff as a priority. Workforce planning and staff retention must all be addressed.
Normally when hospitals cannot cope safely with the budget they are allocated, they apply for “drawdowns” from NHSE, England’s top NHS funding body. NHSE is currently refusing to give such monies to some hospitals. The Health Service Journal commented that “trusts are more likely to have their applications rejected or receive less than they asked for. Major trusts have warned of “slippage” in payments to suppliers.
“An email from NHSE’s finance team, seen by HSJ, said trusts applying for support need to provide assurances from their chair and CEO that they are on track with financial plan; have cash and cost controls in place; and confirm their workforce plans are on track.”
“Confirm their workforce plans are on track” does not mean they are to hire the doctors, nurses, and midwives they need, but the opposite. One whole ICB and their trusts have been sanctioned for recruiting too many staff.
We, with other campaigners across Merseyside, Cheshire,Lancashire and nationally, will keep up the fight to restore and repair the NHS. We will be lobbying Labour’s Conference, in Liverpool, in September. Please help by writing to your MP demanding the restoration and repair of the NHS.
Lets use this opportunity to make the case for a return to the Bevan Model of the NHS
More than 70,000 people have signed our petition to Save Liverpool Women’s Hospital online and on paper. The paper petitions represent 20,000 individual conversations about these issues.Please continue your suport.
The Hospitals in Liverpool, and just in Liverpool, under pressure from the ICB, intend to set up a further layer of “governance” to manage finances and drive some greater cooperation. This committee is called the Adult Acute and Specialist Hospitals Joint Committee. The ICB controls all the finances for hospitals across Cheshire and Merseyside.
We like the cooperation idea, but not the idea of both the specialist hospitals and the Women’s Hospital being in unequal competition with the main hospital services for priorities and funding. Liverpool Women’s Hospital already has an imposed shared CEO, Chair, and other officials with Liverpool University Hospitals Foundation Trust (the Royal, Broadgreen and Aintree), all men, people with no published expertise in women’s health or maternity.
These proposals mean that Liverpool Women’s will have a completely shared board with the Royal, Aintree and Broadgreen Hospitals, and have their decisions further scrutinised by this additional board which will also cover the specialist hospitals in Liverpool. These hospitals are.
Liverpool Heart and Chest Hospital NHS Foundation Trust (LHCH),
The Clatterbridge Cancer Centre NHS Foundation Trust (CCC), and
The Walton Centre NHS Foundation Trust (TWC).
How will women and babies fare in this further layer of bureaucracy? How does this fit in the spirit of the Ockendon report? How will the specialist hospital services fare?
These hospitals serve a wide area, not just Liverpool.
We took twenty thousand signatures to the ICB and were promised consultation.
We were promised consultation on any future plans. Those promises are being broken.
The waste in the NHS is in privatisation and the failed “business” model. The original NHS model, the Bevan model is much more cost effective. The big acute hospitals need better funding and staffing as do the specialist hospitals, though it is not just funding that is needed. We want the NHS restored and repaired.
The evidence is clear. We need more midwives and a better maternity service. Patients need access to GPs, an end to huge waiting lists, access to well-functioning Accident and Emergency care and better cancer treatment. We need to be able to get a dentist’s appointment without our bank or credit cards creaking. There are millions of people on waiting lists. GP services are in disarray and GPs are taking protest action. Mental health services are severely damaged. In Cheshire and Merseyside, 75% of young people asking for help with their mental health get nothing. NHS staff need better pay and much better working conditions.
We need all our children to be well fed, for the good of their health and well-being now, and to prevent chronic illnesses in later life. The UK is the worst country for increasing child poverty. Far too many of us in Liverpool are poor or hard up. This can make us forget that we live in a rich country, one that can afford good public services. For decades Liverpool people fought for health care till we won the NHS. We want a return to the original NHS model where hospitals are not competing but cooperating and pursuing their specialisms. We must insist this new Government funds the NHS and restore it to the original Bevan model that less than ten years ago made it the best health service in the world. Funding healthcare is a great investment for a government to make. It is good for people’s health and for the economy.
Speak up for the NHS.
Talk to your neighbours and family about the NHS.
Join our campaign. Sign the petition if you have not already signed.
It is indisputable that our health service is in crisis and that the NHSE and the Government know full well how bad it is. The purpose of our letters to the ICB is to put public concern on record and hopefully put pressure on the politicians to restore and repair the NHS. We also wanted to ensure that reports were clear and not cover-ups.
There was considerable discussion about the letter below in the public section of the ICB meeting in July. The CEO said that they had asked for £ 150 million in additional funding from NHSE ( National Health Service England)but the Hospital Trusts’ CEOs would have asked for £ 300 million more but he was being realistic. That realism means preventable deaths pain and suffering and exhausted staff.The fault though lies with the government.
Cheshire and Merseyside NHS Integrated Care Board
Our Letter
On behalf of the Combined Cheshire and Merseyside NHS campaign groups
to
Dear Chair and Chief Executive
Re the papers for the JULY 2024 meeting of the ICB
We write once more to express our deep concern about the level of provision for Accident and Emergency Services in this late summer and particularly in the coming autumn and winter.
Last year we wrote expressing our fears that the resources of staff, beds and premises for the winter of 2023-24 would be inadequate. They were more inadequate than we as lay people predicted.
Looking at the papers for July 2024, and particularly the pressure to make 6% CIPs both at ICB and provider levels, we again express our fears that this coming winter will be still worse. The decision of NHS England to send in Price Waterhouse to suggest further cuts is very worrying.
In our stalls and public work, we have come across medical students expecting to have to emigrate on completion of their training simply because of the state of the hospitals. They told us, and this is confirmed by others working in the hospitals, that the overcrowded state of A and E and the overall shortage of hospital beds, means this crisis affects nearly all the wards with patients boarded into already full wards.
We are concerned about the toll this takes on staff. Patients though, are put at risk to their lives and long-term impairment from these conditions. The Royal College of Medicine reported that “Nine out of 10 A&E doctors say patients are coming to harm in UK’s Emergency Departments”.
We saw the report from the Covid enquiry. Our health services must be prepared for future episodes of explosive need.
Your medics have a duty of candour, and you as NHS managers also have a public duty to speak truth to power.
We demand that an urgent plan of action is drawn up, including all available doctors, nurses, midwives, diagnostic services staff, and additional cleaners and health care assistants be employed, that additional physical space be provided, that an excellent standard of hygiene and personal care be provided in all A and E departments, including good food for staff, those waiting with ill patients, and where safe, for patients.
We also demand that the ambulance service be enhanced to make sure patients are reached in good time. We saw parliamentary reports of 500 people dying because an ambulance did not reach them in time.
These patients are our family and friends, our neighbours and workmates.
Urgent and comprehensive action must be taken.
Ensuring that patients are seen by GPs in good time, and by qualified doctors rather than PAs will reduce the number of urgent cases arriving at A and E.
It ill behoves the NHS strategists who made a virtue out of closing hospital beds to now pass the blame to the chaotic and market-driven social care sector, where over decades the few local authority homes have been pressurised to close. Social care does need a major service-driven reform. As with the trains and water privatisations, social care privatisation has not proven to be a service-driven model.
When we talk to people in public the litany of the closed hospitals in Liverpool is frequently quoted, and the reduction in beds with the rebuild of Liverpool Royal.
Such political pressures as we can exert are nullified if your reports do not adequately reflect the extent of the problem or if your reports are written in a jargon understood by a few. We do not need Professor Pangloss mimicked in these reports, but rather a reflection of reality.
We say by all means make better use of the resources you have, but also make the plans that need making to ensure safety even if those plans are knocked back, at least they are ready to go if we as the public can build the pressure to release the funds.
We had written another letter previously and this had caused a stir at the ICB with one trust CEO saying “You thought it was bad for patients! You should have seen what it was like for staff” But still the CIPs(cuts) went through.
The previous letter said
Hello,
I would like to put the following to the forthcoming meeting of the ICB.
How is the ICB preparing for Covid this winter?How will hospitals make preparations
given they are expected to make large cuts(CIPS) as described in the board paperwork.
given there are so many hospitals already on Opel level 3 in summer and early Autumn.
given Staff shortages and unfilled vacancies.
and the number of NHS staff relying on food banks, suggesting weakened responses.
I refer you to the recent enquiry hearings which showed how badly the country was prepared for the first wave, with hospital infrastructure poor. SARS-CoV-2 frequently mutates and causes waves of infection and is to some extent seasonal. It is normal for The NHS to watch levels of Flu infections in the Southern Hemisphere Winter to plan for our Northern Hemisphere Winter infections. It would seem sensible to follow Covid levels similarly. Australia had a large and extended wave in its last winter, as reported in the BMJ 2023; Covid-19: Australia’s future policies will be evidence led after “profound impact” of latest wave, says minister.
How have you taken account of the Australian experience in your preparations for this winter?
I look forward to your response,
The use of corridor care and inboarding is now so common a set of safety advice has been prepared. Those of us who saw the Dispatches programme about Shropshire A and E can see the need for this but there should not be a need for corridor care at all.
Investment in healthcare makes the economy and the people healthier and stronger. There are many sources for this information but we will post just a few.
The government wrongly keeps referring to the household budget as though that is how Government spending works. Damaging our healthcare is about as sane as refusing to pay for your toilet to be repaired when you are hard up.
Our healthcare is ours. We want it back. It does not belong to the corporations. We know that the US corporations run, in the US, the worst health service in the advanced world according to the Commonwealth Fund an authoritative US organisation.
We, with more than 70,000 people who have signed our petition (an online version of the petition can be signed here), oppose these plans but we publish this letter so everyone can see all the details we have on the proposals.
We have been promised earnestly (!)and repeatedly in board meetings that our campaign would be consulted about plans for the future of Liverpool Women’s Hospital. What we got, however, was a leaked copy of a letter to staff written by the joint chief executive of Liverpool University Hospital Trust and Liverpool Women’s Hospital. We will publish our response shortly.
This is the letter
Dear colleagues,
As you will all know, the adult and specialist Trusts in Liverpool have a strong record of working together for the benefit of patients and their families across the city, and the region.
We have a lot to be proud of, for example the stroke pathway service between Liverpool University Hospitals NHS Foundation Trust and The Walton Centre NHS Foundation Trust, the cancer pathways across all Trusts, and improved diagnostics waiting times across the city.
In January 2023, a report called the Liverpool Clinical Services Review recommended we continue to build on this in several key areas to help create a healthier city. Since this report, good progress has been made towards ever further collaborative working across the system.
Next Steps for Collaborative Working in Liverpool
As the next step in this work, NHS Cheshire and Merseyside has asked the five adult acute and specialist Trusts in Liverpool to establish a joint committee. Its purpose is to create sustainable healthcare systems for the future with a clear focus on improving patient care and outcomes.
Staff in all Trusts work incredibly hard and care deeply about doing the right thing for patients. As we all know there are significant challenges facing the NHS – pressures every day, capacity, and funding. And this year is going to be the toughest yet.
We have been asked by NHS Cheshire and Merseyside to come up with a way to act more quickly, find solutions and have a simpler way of making decisions about things that involve us all with a clear focus on improving patient care and outcomes.
Adult Acute and Specialist Hospitals Joint Committee
The Chairs and Chief Executives of the five adult acute and specialist Trusts, outlined below, will sit on the joint committee:
Liverpool Heart and Chest Hospital NHS Foundation Trust (LHCH),
Liverpool University Hospitals NHS Foundation Trust (LUHFT),
Liverpool Women’s NHS Foundation Trust (LWH),
The Clatterbridge Cancer Centre NHS Foundation Trust (CCC), and
The Walton Centre NHS Foundation Trust (TWC).
This will enable more streamlined decision making and help to build upon existing collaboration with a specific requirement to collectively manage the financial position across the Trusts, deliver economies of scale and manage vacancy controls
The focus of the joint committee will be to establish the new governance arrangements, meeting in shadow form (i.e no formal authority) in September 2024 and be in place formally (i.e. with authority to make decisions) by April 2025.
Over the coming weeks the detailed delivery plans are being developed. I am committed to ensuring colleagues are updated as more information on the joint committee plans becomes available. Colleagues at the other Trusts are also receiving this information today.
Shared Board of Directors for Liverpool University Hospitals NHS Foundation Trust and Liverpool Women’s NHS Foundation Trust
Additionally, LUHFT and LWH are building upon their existing joint board appointments and are working towards developing a shared Board of Directors. This supports Liverpool Women’s Hospital’s long-stated ambition to be aligned to a larger acute Trust to support the management of identified clinical risks.
Work is underway to develop the detailed plans for establishing the joint board by late Autumn 2024.
The Women’s Hospital Services in Liverpool Programme, commissioned by NHS Cheshire and Merseyside will continue to progress with developing proposals for safe, high-quality maternity and gynaecology services in Liverpool through public consultation and engagement.
These new governance arrangements will not impact on the delivery of services at the respective hospital sites or on this established programme of work.
Keeping you updated
We will keep you all informed as much as possible through regular Trust-wide communications and through your line managers. We know that many of you may have questions in relation to this subject. We have drafted some initial FAQs that you may find useful. ( this link is better: our edit)
If you have any further questions, please send them to communications@liverpoolft.nhs.uk – to help inform updates to the FAQs, further communications and briefings.
The author is James Sumner Chief Executive of Liverpool Universities Foundation Trust and of Liverpool Women’s Hospital
The Save Liverpool Women’s Hospital campaign will publish a detailed response as soon as we can do so with real consideration of the risks involved in these proposals. Meanwhile please keep campaigning to Restore and Repair our NHS so such dangers to our healthcare are removed.
For all our mothers, sisters, daughters, friends, lovers and every single baby, Save Liverpool Women’s Hospital. Restore and Repair the NHS
“Do not appeal, do not beg, do not grovel. Take courage, join hands, stand beside us, fight with us”!
The Suffragettes knew how to campaign and so do we.
This post is being written just two weeks after the General Election which saw the Conservatives, who had so very severely damaged our healthcare, thrown out. (Hurray!)The new Labour Government has a massive majority but lacks a clear plan to restore and repair the NHS, and talks of more privatisation. They also have form in bringing in privatisation in earlier governments. So, we need to review the situation and renew our campaign.
We are far from alone. There are campaigns like ours dotted around the country. The NHS is immensely important to people in the UK.
Our online petition says Save the Liverpool Women’s Hospital. No closure. No privatisation. No cuts. No merger. Reorganise the funding structures, not the hospital. Our babies and mothers our sick women deserve the best.
We fight too for the whole NHS; the issues are inseparable. Maternity is one of many issues, including the overall reduction in healthcare capacity in this country as seen in the many hospital closures, shortage of doctors, multiple kinds of privatisation, the use of the business model, and the influence of big US “health” corporations. We, though, focus on maternity and our local issues (as well as the big national and international healthcare, women’s rights and children’s rights issues.)
From the start we said
For all our mothers, sisters, daughters, friends, lovers and every precious baby save Liverpool Women’s Hospital and the NHS.
In the years we have been campaigning we have seen severe damage to maternity care nationally, and to the whole NHS. Mothers and precious babies have paid a heavy price. Highly qualified people have conducted report after report into the situation and the last government gave lip service and let the situation deteriorate. These are heartbreaking and infuriating descriptions of some maternity in the UK.
The most useful definition of birth trauma we have found is this.
“A traumatic childbirth experience refers to a woman’s experience of interactions and/or events directly related to childbirth that caused overwhelming distressing emotions and reactions; leading to short and/ or long-term negative impacts on a woman’s health and wellbeing.”
There is support in issues around Birth if you contact the Birth Trauma Association, and sometimes through the maternity hospital. Liverpool Women’s Hospital has a service called the Rainbow Clinic for women having a baby after an earlier traumatic experience, normally involving the death of a baby but it is not advertised on their website.
Some mothers thankfully do have great experiences of birth but the numbers reporting far from good experiences is heartbreaking. The racial and class divides in Maternity outcomes are scandalous. Maternity is grossly underfunded and understaffed. The staff are overworked.
Continuity of Carer where pregnant women are cared for by a known small team of midwives from the pregnancy through birth and the post-natal period would help if it were fully staffed and funded would help. Without funding and staffing, the attempt to introduce continuity of care caused chaos. Donna Ockendon’s report called for it to be halted until full funding and resources.
We are concerned about women’s experience of delayed induction of labour and its link to emergency caesarean sections.
Staff in our hospitals and community teams work hard with inadequate resources and inadequate staffing. We will shout from the rooftops”We need more midwives.”
We have seen NHS managers looking for all kinds of magical thinking solutions to the problem but Liverpool Women’s Hospital does not need a new building, we do not need new fashions in childbirth, we need women’s choices to be heeded, we need more midwives, more obstetricians, more anaesthetists, more natal nurses, more health visitors, more infant feeding specialists. We need better blood services, well-maintained buildings, better food for staff at night, we need bursaries and we need to retain the staff we have. Above all, we need more midwives.
It would be nice if NHS managers were prepared to speak truth to power but we know that bullying is endemic in the NHS.
Many reports, especially in the right-wing press criticise “NHS Maternity Care”. However, the US model of maternity care is the worst in the developed world so no lectures from American Health Corporations or their UK offshoots or employees or political servants, please.
We must make the politicians listen. Our campaign must become deafening.
We took a big Restore and Repair the NHS campaign van around Cheshire and Merseyside in the week before the election. We went to Leighton Hospital near Crewe and up to Southport, to Ellesmere Port, to Chester, to Neston, to Warrington, to Kirkby, Whiston, Birkenhead, West Kirby and Liverpool. The van was met by campaigners in many places and had good support from the public. We heard stories of gratitude to the NHS and stories of long waits and being unable to access treatment.
We were not supporting a particular political party but we were opposing the last government and all the previous ones that had damaged our healthcare in the name of austerity or the discredited idea that private companies could run public services better than public services.
The NHS was one of the biggest issues in that election but too many people felt there was nothing they could do about it. We saw the lowest turnout in the election, the lowest since ordinary people had the vote.
One conversation comes to mind, one in Ellesmere Port Market(a great place!). A woman said there was nothing they could do about it however bad it was. We said that the suffragettes managed to change things, without even having the vote, that slaves got slavery abolished, that we do not send kids up the chimney anymore, and that the fight for the NHS was from the people not from political parties.
We also want to do a shout-out to the Lodge Lane food pantry, a great crowd of people who gave our van a real welcome.
It would be so much better if Repairing and Restoring the NHS was once again a serious commitment from one of the political parties but it still is not. We must make the issue of restoring and repairing the NHS such a big campaign that politicians must listen.
The NHS needs proper investment NOT “reform” and privatisation. This campaign joins with NHS workers Say No in saying #Wes change your plans #no to NHS privatisation.
Our campaign is part of a wider campaign in Cheshire and Merseyside to restore and repair the NHS. The local ICB we know is short of funds but now has been told to bring in a private company to look at how it can reduce costs. This is ridiculous. Liverpool Women’s Hospital requires additional funding to keep safe. Funding comes through the ICB. We are far from the only hospital or service in that situation. It is an intolerable situation and we call for public support to stop this dangerous nonsense. The lives and health of our precious babies and the health and at times lives of their mothers depend on improving the healthcare.
We warned the ICB that last winter would be dreadful in the NHS and dreadful it was. We need urgent action now to prevent another set of winter problems in this area.
Our hearts go out to the women and children of Gaza, especially to the pregnant and new mums. Cry justice for the dead and injured. We weep and rage with the patients whose doctors and health workers who have been willfully killed by Israel or tortured in Israeli prisons in this terrible onslaught. We mourn too the dead of Ukraine and those in all the other conflict zones.#CeasefireNow#StopGenocide#SavetheChildren.
With your help, in person or through donations, we will grow our NHS maternity campaign so it cannot be missed. Remember every campaign requires people to talk to their friends about the issue. These little conversations are the seeds of success.
What can you do?
1 Talk to your friends and workmates about the need for a fully funded publicly owned NHS.
2. Get involved with the campaign personally.
3. Tell us about your experiences and suggestions
4. Make formal complaints about poor service to the hospital and to your MPs and councillors. We can help.
4. Get your union branch or other organisation involved in the campaign. Ask us to send a speaker.
5 Give out leaflets in your street.
6 Put up posters.
7 Come to our events. Look out for events when the Labour Conference comes to Liverpool at the end of September.
Speak out for the NHS. The NHS matters in this election and after it.
Don’t leave it to the politicians.
The NHS came from the people and the people must organise to get it back!
Restore and Repair the NHS.
Cheshire and Merseyside NHS campaigners are taking a campaign van around the area to remind people of the need to Restore and Repair the NHS.Politicians should heed the needs of the people before the needs of the banks
This article gives information gives more information than the leaflet we are giving out
We say to any government, you must repair the damage of the last two decades, and rebuild the service after years of cuts. The capacity of the NHS to provide adequate timely treatment was cut as the population aged. But it made big money for the very rich. We want the NHS back for the people, not for profit.
Join our campaigns until the politicians restore and repair the NHS.
The Royal College of Nurses has declared a national emergency in the NHS.
Doctors are warning of large numbers of avoidable deaths from NHS shortages.
Life expectancy in Cheshire and Merseyside is lower than the national average for men and women. Access to health care is crucial in this. Will you willingly give up years of your life, and the lives of those dear to you, to fund privatisation and poor healthcare?
The NHS is underfunded. Our local Integrated Care Board said in May 2024 that “provider financial plans exceed the level of funding available” Providers are hospitals. The hospitals have huge waiting lists and dreadful A&E waiting times. They need the money. Maternity desperately needs funding.
The damage to the NHS has been deliberate. Privatisation, underfunding, deskilling staff, closure of hospitals and beds, organisational “reforms” using expensive financial consultants, PFI, and poor building maintenance; it all adds up to Government policy and it has been lethal.
Privatisation involves public money being paid to private companies to provide a service and allows the private company to make a profit and to deny care to some patients. That profit is money that could go to the public service. They are not more competent nor more efficient. £10 million pounds a week goes to private profit according to We Own It. The ICS structure is based around “commissioning services” pushing ever more of the NHS budget into the private sector.
Fund and staff maternity services to equal the best in Europe. We need more midwives. Can we say that again? We need more midwives. Did they hear that? Say it again WE NEED MORE MIDWIVES. There have been so many reports on the state of maternity services, we need action now. Women and their families are angry about what’s happening in maternity.
Children’s Health
The health of our children is worsening. Ensure every child has timely access to full healthcare, at birth, in the community, at the GP surgery, at Accident and Emergency, and in planned care in the hospital. Bring back health visitors.
GPs
The GP service must be restored and be staffed by qualified doctors. The government must allow spending on doctors as well as ancillary services. A good GP puts years on your life. GP services have been cut with overall funding cuts of 20% per patient per year since 2016.
Mental Health Care
Mental health services must be renationalised and brought back into the NHS and staff trained and paid to NHS standards. The damage is disgusting.
Dental Health Services
Everyone has (or did have) teeth. Our dental health services must be made available to everyone. The damage is immense. Change the contracts to ensure this. Bring back NHS dentistry.
Hearing Services
Audiology must be brought back in-house to make sure everyone has access and no one has to pay privatised prices. Hearing aids are free on the NHS if you insist on using the NHS. These hearing aids are just as good as the ones for which people pay hundreds
Ophthalmology
Eye health services must be brought back into the NHS to ensure quality of service, and access for all and to prevent unnecessary treatments that make profit. When so much of the service is farmed out to for-profit companies and the NHS just does the most complex the whole training system fails
A&E
Accident and Emergency Services. Waiting for hours in A&E is an awful experience as is being treated in a corridor. According to new estimates, long waits in A&E departments may have caused around 30,000 ‘excess deaths’ last year. The stress on staff is also unbearable. We say No more winter crisis. Employ the staff, provide the buildings, and open more hospital beds.
Healthcare for all, free at the point of need. End the policy of charging for some services, reduce prescription costs, and stop discrimination against migrants, who pay twice for the NHS and are charged at 150% of costs yet pay all the same taxes as everyone else.
Our data
The NHS as a national service for over 75 years is gold dust as far as big data companies, health insurance companies and the US health corporations are concerned, the information about our health care, our symptoms and treatment must return to being confidential. Palantir has been given a huge sum of money to manage our data. Kick out the big US data firms and the other private firms who are getting rich off of our data.
Staffing
All vacancies in the NHS must be funded and recruitment processes must be positive and wide-reaching, including winning back many nurses and midwives who have left. Say no to two-year trained staff, no to the use of Physician Associates except in situations where they are in real-time supervision. Workforce planning must be based on training and employing more qualified doctors and nurses to meet the needs of the people. Student debt in medical nursing midwifery and allied professions must be abolished, and bursaries re-introduced so ordinary people can afford to train.
Pay the NHS and social care staff well. This will help keep staff and reduce their stress.
Social care
Social care covers services to the frail elderly and to disabled people people of all ages both at home and in care homes. Councils are starved of funds and stupidly went along with the policy of privatising their own care homes. Now care homes are privately run, by for-profit companies and do not provide a universal service but a service where and when they can make big profits. Most are privately owned by big companies and hedge funds. This is more public money going to shareholders. Neither are care services free at the point of need but charge large fees to users who do not qualify for NHS funding or Local Authority funding. Children’s social care is in a shockingly bad state and adult social care needs radical reform. If you are interested in this area see the End Social Care Disgrace campaign
The private sector. This is no solution to the healthcare crisis. They don’t have the full range of treatments or facilities and are dependent on the NHS for backup. Most doctors who work in the private sector also work in the NHS. The NHS has103,277 general and acute beds while the private sector has about 11000
We all need healthcare. The need for the NHS is crystal clear. All the parties say sweet words about protecting the NHS, but we have to hold them to these promises. (bar one- Reform wants to bring in an Insurance/market-based system)
The NHS is the most cost-effective structure and the most equitable system for healthcare.
Give the NHS an immediate boost to its funding.
Renationalise the NHS. Make it once again a national service. Stop privatisation.
A healthy population is obviously more effective than one with millions of people waiting for treatment. Millions of people denied treatment or kept waiting for years is morally unacceptable and bad economics.
The incoming government must fund the NHS to prevent the next still worse winter crisis. It must address the issues around maternity, GPs, dentists and NHS pay, or the people will be very angry, just as the current government is blamed. It took many years to win the NHS and might take years to win it back but the campaign will go on if you give it your support
The campaign to restore and repair the NHS must go on !
Save Liverpool Women’s Hospital, the national maternity service, and women’s and babies’ healthcare. While we fight for Liverpool Women’s Hospital, we fight also for the whole NHS.
“As we go marching, marching We battle too for men For they are women’s children And we mother them again.”
Together ordinary women and men can make a difference, and can put huge pressure on the government to improve our services and maintain that improvement. We cannot leave it to election promises, especially as neither main party at present is supporting the full restoration of the NHS.
Our campaign focuses on Liverpool Women’s Hospital. So, we asked local pregnant women for their thoughts.
“I think the most basic thing that women giving birth need is to feel safe, and to be able to have confidence and trust in the people who care for them before, during and after the birth of their baby. Continuity of care is so important, and while this is challenging to deliver, this should be the goal wherever possible. The Women’s has suffered some serious problems in the recent past, and work needs to be done to restore trust and confidence for the women and families who rely on this vital service. Women need to be able to access midwifery-led care, and be supported in their choices around birth and beyond. I want to feel secure that I will be offered treatments that will be beneficial (nothing unnecessary), that the midwives and doctors will listen to me and answer my questions, that they will seek my consent before they intervene, and that the quality of care and communication will be consistently of a high standard. I have experienced both excellent care and coercive and traumatic care at the Women’s in the past. I understand that there are serious system pressures that affect staff throughout the trust, but no woman should leave the postnatal ward feeling traumatised and vulnerable. Staff need all the support and training necessary to ensure this does not happen. Research demonstrates that birth trauma is a national problem, and I would like to see the Women’s taking a leading role in addressing this silent epidemic. As a tertiary centre and leader in obstetrics and foetal maternal medicine, the Women’s should be setting standards, not struggling to meet them.”
Another comment was:
“We need more focus on women with complex social needs as they have terrible experiences once they go in to deliver.”
We agree and say.
Fight to save and improve Liverpool Women’s Hospital.
Restore and Repair the whole NHS.
We need a national health service, funded at least as well as other European Countries, publicly provided, not for profit, available to all humans in the country, free at the point of need. This model is the safest and most economical model of healthcare. The US have a dog’s dinner of a healthcare model but it costs much more than the NHS and has many more preventable deaths.
The UK does not spend enough on our healthcare and wastes billions on private profits.
Governments know this and choose to involve big US corporations in the NHS so they can make a fortune, as our service runs on empty. The years of closures and mergers have done great harm and the last thing we need is more health care corporations to rip us off.
The U.S. has the lowest life expectancy at birth, the highest death rates for avoidable or treatable conditions, the highest maternal and infant mortality, and among the highest suicide rates. The U.S. has the highest rate of people with multiple chronic conditions and an obesity rate nearly twice the OECD average.
Liverpool Women’s Hospital requires about 25% more funding. This is because eighty per cent of its work is maternity, and maternity is badly funded nationally. However, funding for the whole ICB (NHS) in Merseyside and Cheshire is also a problem. One of the hospitals that cannot safely work within the given budget is Liverpool Women’s Hospital. The Board of Liverpool Women’s Hospital has set a budget for safety and must be supported in this.
The Cheshire and Merseyside Integrated Care Board provides the bulk of funds to the hospital with a small amount coming nationally from funding for specialist services. The ICB in turn gets its funding from NHS England. NHS England funds maternity through what they call the maternity tariff. This maternity tariff is inadequate for safe care. NHS England gets its funding from the Government. The buck stops with the Government.
The ICB said it has serious funding issues in its most recent report;
“Colleagues will be aware that the financial planning round for 2024-2025 has yet to be concluded. This is largely because provider financial plans [providers are the Hospitals and non-hospital trusts our comment] exceed the level of funding available and we remain in an iterative process [iterative means going back and forth] with NHS England as we seek to find the right balance between further cost improvements [cost improvements means cuts] and maintaining the core quality of services. 5.2 At the time of writing this report we were forecasting a deficit for the year in the order of c£150million (2.24% of turnover). We will be able to report back to Board verbally at its meeting in May [This meeting was cancelled].”
Sadly, Maternity does not feature in the priorities of the ICB despite reporting that many more women experienced a delay in induction of labour. This means that a woman has been told that her baby needs to be born soon and has come into hospital, to have the baby and then is kept waiting (and worrying) for more than 12 hours.
The NHS came from campaigns over many years from ordinary people, from trade unions in mining towns and working-class women’s organisations especially the Cooperative Women’s Guild who left behind a great record of their work in 1916 in the book ‘Maternity: Letters from Working Women, Collected by the Women’s Co-operative Guild’. Eventually, Nye Bevan founded the NHS as part of the 1945 Labour Government. It dramatically improved women’s survival giving birth, and the survival of babies.
Linked problems.
Women and children have been hardest hit by austerity and this has affected our health The prospects are grim indeed. In Liverpool “The life expectancy of women will fall by one year, and they will be in good health for 4.1 fewer years than they are currently. Although they are starting from a lower base, men will live 6 months longer than currently, and more of that time – 1.8 years – will be spent in good health.
Tell everyone who wants your vote to commit to real improvements in maternity services, a real commitment to the NHS. But do not leave it to MPs, get involved in the campaign to restore the full NHS and Maternity care. Suffragettes did not have a voice in parliament but they made themselves heard. We can campaign as well as our great-grandmothers.
Save Liverpool Women’s Hospital. No mergers, no dispersal of services. We need more midwives. Fund all the maternity hospitals well. Staff them well. Staff should not be pulled from ward to ward just to manage day-to-day demands. Each ward should be well-staffed. Fund postnatal support. Fund safety-critical improvements. Fund and staff the specialist work of Liverpool Women’s Hospital. Make treatment timely and safe, without long waits for induction of labour. Make maternity services improve women’s mental health not damage it.
We need more midwives, and midwives need a professionally safe workload and good pay. It is hard to stay focused professionally if you are not sure where the next meal or heating bill is coming from or if you are working extra shifts to make ends meet.
“Do not appeal, do not beg, do not grovel. Take courage, join hands, stand beside us, fight with us.”
It takes a weird level of cruelty to cut services for the birth of a baby but that is what has happened. Our campaign is far from alone in raising these issues. The government knows quite well what is happening in maternity. Multiple national reports have shown the crisis in maternity services for mothers and babies. These are some of the reports, all reported to Parliament.
The government responded with endless cuts to the NHS budgets. This year’s funding allocation for the NHS in real terms, taking into account inflation, is the worst in many years.
Improving maternity outcomes needs to be everyone’s business. Let us make it our business.
There are other NHS problems. Mental health care has been sliced, diced and privatised. Dentistry is simply unavailable to many people; GP services are in serious trouble through underfunding and crazy schemes to reduce our contact with a GP. Meanwhile, reports show that having contact with the same GP adds years to our lives
The service must respect and work with mothers. There should be continuity of care, not an impersonal production line.
It shows how the US right-wing policies that restrict abortion inflict terrible damage on women’s bodies, mental health, and rights.
“My heart is broken: As friends & family know, my wife was pregnant with our 2nd child, & about to begin her 2nd trimester. A few days ago she had severe pains, & bleeding, and had to go to the emergency room. There, it was discovered that our baby no longer had a heartbeat. Devastated doesn’t come close to what that feels like. Unfortunately for people like us, because of the current laws in the state of Texas, that was only the beginning of this nightmare. Jess (my wife) had an “incomplete miscarriage”, and what needed to happen, what was best for HER, and her health, was to terminate the pregnancy, and get the baby out. The doctor gave her a medication that would move this process along, and sent her home. Where, apparently we would be handling it ourselves. We were told it might take a couple of attempts before it worked. I’ll let you decide how you feel about that. After a long, painful night of the equivalent of early labor, the baby was still with her. So, we went back to the Emergency Center to get the 2nd dose. A new doctor was on call. He was an older man. You could hear him in the hallway as he said, “I’m not giving her a pill so she can go home and have an ab*rtion!”. Being well aware that our baby no longer had a heartbeat. Then, he came into the room to say, and I quote: “Considering the current stance. I’m not going to prescribe you this pill”. Then, just sent us on our way. The “CURRENT STANCE”?! Did he really just say that?! No one should ever have to hear their wife say: “Get this dead baby out of me!”. Can you even imagine how that must feel? The pain, and the bleeding continued. So, we decided to go to another hospital, about an hour away. There was a female doctor on call there, and we thought we might have better luck. I should probably mention, the procedure to get the baby out is called a D & C. It’s scary, & traumatizing, but sometimes necessary in situations like ours. Especially in emergency circumstances. So we get to the next hospital. They take Jess in, ask her a bunch of questions, do a new scan… confirm that the baby is still there, with no heartbeat, and then disappear… for hours. Only to come back in and keep asking the same questions over and over. It’s becoming clear that they’re primary concern is NOT my wife’s health. Instead, they seem to be worried about the legalities involved. So, they decide it is not “enough of an emergency” to perform the D & C. They do, however, prescribe another, stronger, final dose of the medication for us to try again… at home. So, we go home to try again. Another long day/night of early labor pains. Only to discover my wife UNCONSCIOUS in the bathroom. Having to pick my wife’s cold, limp body off of that bathroom floor, not sure if I was about to lose her, is something I will NEVER forget. She had to be rushed to the hospital. By this point she had lost so much blood, and bodily fluid, her body gave out. They were able to stabilize her, give her the fluids she needed, and we came back home yesterday afternoon. We were also able to confirm that our baby was no longer with her. Now, not only do we have to live with the loss of our baby… we have to live with the nightmare of what we just experienced because of political and religious beliefs. MY WIFE’S HEALTH SHOULD HAVE COME FIRST. PERIOD! God knows what mental and emotional damage this has done. If you consider yourself a staunch “pro-lifer” … 1) You’ve never been through what we just went through, and 2) You should take a long, hard look in the mirror and reevaluate your reasons for supporting such a cold, barbaric, ignorant point of view. It’s not that black & white, and it’s never going to be. If you think your “Pray To End Ab*rtion” sign in your yard is “Christian”, I suggest you revisit the teachings of Jesus and try again. If you support these laws that make ab*rtion illegal, and result in people being put through what we just were, you should be ashamed of yourself. I’ve never been so angry, or heartbroken… and the devastation I’m feeling must pale in comparison to what my poor wife is feeling.
Take the fight for the NHS into all our workplaces. Make repairing and restoring the NHS a topic of conversation at work. Blow the whistle on the damage to our NHS. There are nearly thirty-three million people at work in the UK. More than 6 million of those workers are in a trade union. Talk at work also gets back into the community. People at work are powerful. Make the NHS the talk of the workplace.
Support the NHS workers.
The magnificent work and skill of NHS staff just about keep the hospitals functioning and saving lives and health day after day, but there is a terrible toll on lives caused by Government policies on on the NHS with almost 300 avoidable deaths a week attributed to the situation in our Accident and Emergency units.
Who was Nye Bevan?
Nye was a miner and strong trade unionist who became an MP in 1929. He retained his loyalty to his class through his political life. In the 1920s there was no national health service. In the mining areas limited health services were organised by subscriptions collected by the miners, but such services were not available elsewhere. Working-class families often had no access to healthcare, especially for women and children. There was a huge demand for better healthcare from the unions, working-class women’s organisations and other organisations of the labour movement. Nye was part of that pressure. In 1945 after World War 2 Labour won the general election and Nye became Minister of Health. Against much pressure from the establishment, Nye set up the National Health Service.
The national health service was free at the point of need, paid for by taxes, and available to everyone, rich and poor young and old, every religion, every colour. It was a coordinated national service, providing all the available treatments. GPs and hospitals, baby clinics and public health. The NHS made a huge difference to working-class lives and especially in the lives of babies and women giving birth Until 2017 it was the best health service in the world. You can find out more in Ken Loach’s film Spirit of 45
How people at work can help win back the NHS?
Talking to other people at work is a powerful way to spread the campaign and to counter Government and press lies. Every great campaign starts with one-to-one conversations. The media does not report the crisis in the NHS at all accurately. Spreading the word at work can make a huge difference.
We can build solidarity across working people to restore the NHS
Solidarity: Unity or agreement of feeling or action, especially among individuals with a common interest; mutual support within a group. ( Oxford Dictionary)
Workers on the railways, in the water industry, in power, and in telecoms already understand the damage of privatisation.
It is working-class people who suffer most from poor healthcare. Working-class people live shorter lives and are more likely to have long-term health conditions, and these health conditions tend to be more severe than those experienced by richer people.
Maternity suffers badly from these policies as many posts on this blog show. This underfunding is costing lives and most of those lives are those of the babies from the least well-off areas.
Much wonderful healthcare is still available in the NHS, thanks to the huge sacrifices made by NHS workers but the damage is real. Nearly ten million people are waiting for healthcare, while US health corporations are profiting.
The Government spends 18% less per person on healthcare than the average in the EU, and less than half what is spent in the US, where health is much worse. The NHS system is cheaper and more effective than privatisation.
Funding for health services in England comes from the Department of Health and Social Care’s budget. The Department’s spending in 2022/23 was £181.7 billion. This money is a honeypot for privatisers and local and international health companies.
Join your voices for our health care. Demand it back. Demand better!
The healthcare system in the United States is appalling. However recent governments have supported bringing US health corporations into the NHS. In the US health insurance costs about as much as the mortgage and does not cover everything. Many millions go without. “The U.S. has the lowest life expectancy at birth, the highest death rates for avoidable or treatable conditions, the highest maternal and infant mortality, and among the highest suicide rates.” Despite this failure, it is the US model of healthcare that is being brought into the UK by the government. “NHS monies are flowing to private companies, including firms with a dismal track record in the UK and some whose US parents have faced multi-million-pound penalties from state and federal authorities“. Centene, Operose and United Health are all big US names involved in the privatisation of the NHS, including owning GP practices.
Trade Unions and working-class women’s organisations fought to found the NHS and those organisations can help to win it back. Demanding universal healthcare free at the point of need must have sounded far-fetched in those early years of campaigning. It is hard work today too but we can do it.
Private healthcare cannot be as good as a national comprehensive service. It is a far worse system in the USA. Private healthcare has to make a profit. A barrister who got cancer found his private health insurance premium doubled to £163,000 per year.
Profit-centred policies, hidden behind sweet words are reshaping our health services.
These policies are destroying our services, providing fewer services, fewer beds and massive staff shortages. But it provides more profit for health corporations and management “consultants”.
Reverse privatisation, charging, service cuts, closures, understaffing, down-skilling, low pay, and lethal waits for treatment.
The privatisation lobby is infecting Labour too, so the fightback is down to us all.
Everything I’m hearing is that they (Labour) will kick-start private sector investment much more proactively than the Tories were able to do” Henry Elphick, deputy chair of the European Healthcare Investor Association, an umbrella organisation for private capital providers investing in healthcare
The Conservative government has restricted funding, not met pledges about building new hospitals, and indeed closed more hospitals. It failed to maintain and repair existing hospitals, and promised many more GPs and now we have fewer GPs , but they have fed money into the pockets of big business.
Thanks to Government policy, the NHS is short of staff, yet newly qualified doctors and those who have finished their training to become consultants cannot find work. Many NHS staff leave because of the stress at work and poor pay. This is whilst patients wait in pain.
We want to make the NHS once again a great national, comprehensive, universal service, publicly owned, publicly provided, providing timely care, free at the point of need. Good health care is an excellent national investment in the health happiness and wealth of its people.
Demand a return to the original NHS, once the best in the world. (This is according to a regular survey from US Think Tank the Commonwealth Fund.) The health minister once had a legal duty to provide for the health of the nation but that was removed in the 2022 Act
They got rid of the legal responsibility to provide for our health “The Secretary of State must continue the promotion in England of a comprehensive health service designed to secure improvement—(a)in the physical and mental health of the people of England, and(b)in the prevention, diagnosis and treatment of physical and mental illness.”https://www.legislation.gov.uk/ukpga/2012/7/section/1/enacted
The NHS Government funded, providing timely healthcare for all, including all the services, publicly delivered by qualified staff with decent pay and conditions, as designed by Aneurin Bevan.This is the cheapest, most cost-efficient and humane way to provide health care.
Kick out all privatisation. Every penny of government health spending must go to patient care, to the staff, to equipment and buildings, not a penny to the privatisers’ huge corporations. Expand the services. Demand timely treatment for all, rich and poor, young and old.
According to BMA research, the number of doctors per 1,000 people in England is 25 years behind comparable OECD European Union nations, second lowest only to Poland.
The Government has brought in a US-style, service-cutting system through the 40+ ICBs. This redesigns the NHS on US lines and diverts funding (especially from our hospitals) to reward those who cut them back. Fewer services are being provided in the NHS, as the needs increase. Pressure is put on patients to use private healthcare.
If YOU spread the word, we stand a chance of getting our services back.
Government policy costs lives, especially the lives of working-class people. It means avoidable deaths and more years of ill health.
What has happened to dentistry and mental health services can happen to every service. Wages and conditions in the NHS have fallen in real terms. Staff are working way beyond their duties just to keep the service afloat.
People power can be very powerful. That’s how many changes have been achieved
End the “I.C.S.” There are now 42 Integrated Care Systems across England. These bodies are not Integrated, don’t control Care and are not a real System) This model is designed for cuts, privatisation and damaging restructuring.
The NHS model is more cost-effective, and more efficient than the US model or social insurance models. However, no model of health care can run effectively if it is being ripped off by big business and denied adequate funding.
Union members working together will be heard
The NHS is your inheritance yet it is being taken from you. Make sure you leave a functioning NHS to your children and grandchildren
How to fight back for the NHS #Spread the word. Talk at work. Spread the word in the communities. Challenge elected representatives #Talk to one workmate about this each week #Raise the issue with your union. #Challenge the government lies, Challenge the private healthcare lobbyists in the Conservative party and those in Labour #Demand a full-service NHS
They say we can’t afford the NHS. Oh yes, we can!!
Excuses for poor healthcare that are straight lies
Lie 1. The NHS has problems because we have so many old people. Nonsense. The government has known how many old people there would be for decades.
Lie 2• The NHS just needs more funding just needs more funding. No, the money has to go to patient care and staff pay not into the pockets of companies like Optum.
Lie 3 The UK can’t afford the NHS. Nonsense! The UK is the 6th largest economy in the world and good healthcare makes it richer
Multi-national companies are gloating over the Americanisation of the NHS – and the fat, fast profits they can make at the expense of the sick and dying
There is another aspect of privatisation is the bringing in of the US model of Accountable Care. The US government pays big companies for some people’s healthcare. The companies make their profit from the difference between what they get from the Government and what services they provide.
Of course, the final form of privatisation is when people have to pay for all their treatment. Some people already have to pay for treatment in the NHS at 150% of cost. Women giving birth can be charged £14,000 to give birth.
Make the NHS the talk of the workplace.
The Women’s Cooperative Guild were working-class women who campaigned long and hard for healthcare publishing a famous book “Letters from Working Women” in 1916. The banner is in the Museum of Liverpool Life
This article is written on behalf of the coordinated NHS campaigns in Cheshire and Merseyside which includes the Trades Councils in the area, Unite Community branches, Keep our NHS Public, Save Liverpool Women’s Hospital, Socialist Health and other groups. We can help with leaflets, posters, speakers and information Please Contact us via saveLWH@outlook.com or by mail to Save Liverpool Women’s Hospital Campaign c/o News from Nowhere, 96 Bold Street Liverpool
For all our sisters,mothers, daughters and babies.