We fight for Liverpool Women’s Hospital and to Restore and Repair the NHS.
Day by day, the NHS provides services for patients often with great skill and good humour. Despite years of cuts, the NHS survives but it cannot provide all services we need because of austerity and the privatisation agenda.
We are in grim times, but the fightback is growing. Our petition has reached 76,000 signatures. We have had support to pay for our leaflets and meetings. People who spoke at the engagement meetings unanimously supported keeping Liverpool Women’s Hospital. Not a single member of the public spoke in favour of closing it, or dispersing its services. We have great support from the public, and two Liverpool MPs, Kim Johnson and Ian Byrne, have helped this week. The same day as the ICB meeting and the first joint board meeting of LUHFT and Liverpool Women’s Hospital, Kim Johnson raised the issue in Parliament. Ian Byrne sent a great letter to the Engagement Team, saying “NO!”.
However, the process decided by NHS bureaucrats rolls on. We can stop it if we organise.
The many people who have said “that will never happen” should join the fight back.
Two quotes show the seriousness of the threat we face
At the October 9th meeting of the ICB Fiona Lemens, leading the process said, introducing the engagement, “It’s too early in the process to speculate about how services might look, in the future at the Crown St. site and across the city, because we’ve not started that design work yet, but what we can say is that we need that hospital at Crown St. The things that we could consider that we currently need space for would be out patients, day case procedures. We’ve invested in a CDC, we need that diagnostic capacity for the patients in Liverpool, and this is an excellent building to provide that from and we are absolutely committed to NHS delivered services being delivered from that site, and there are no plans to discuss any other forms of services going in there.”
So, Fiona, where will our babies be born? Where will the women of Liverpool receive their gynaecology care? Where will fertility go? Where will genetics go?Where will the Bradford clinic go?
The website for Liverpool Women’s Hospital says about the second strand in this threat to the integrity of the Women’s Hospital, the largest maternity facility in the country :
“From 1 November 2024, Liverpool Women’s NHS Foundation Trust became part of NHS University Hospitals of Liverpool Group (UHLG). UHLG has been created through the coming together of Liverpool University Hospitals NHS Foundation Trust (LUHFT) and Liverpool Women’s NHS Foundation Trust (LWH).
Please note, Liverpool Women’s Hospital is now represented on the Group Board of Directors of NHS University Hospitals of Liverpool Group (UHLG). Details of past Liverpool Women’s NHS Foundation Trust public board meetings can still be accessed via the links below.“
On Thursday 28th November 2024, two crucial meetings happened. These meetings were:
1) The ICB meeting which received the first report of the Engagement process to decide the future of the Liverpool Women’s Hospital, discussed the winter crisis, and how to handle their lack of adequate funds. We, as members of the public, asked questions. We were told that the first response to the engagement would be reported in February or March. They are paying £24,000 to a company called Hood and Woolf to produce the report on the engagement.
We also learned of the grim financial position, and the situation regarding the terrible winter crisis, likely to be worse than last year. There will be a full report on this in a later post.
2) The inaugural meeting of a new joint committee, which has the delegated powers of the boards of Liverpool Women’s Hospital and the Liverpool University Hospital Foundation Trust (which covers the Royal, Aintree and Broadgreen). We fear that maternity will be treated as badly as maternity has been treated in so many other big acute hospitals, leading to major problems and major enquiries.
This joint committee of LUHT and LWH, also reported that the winter crisis is starting (staff tell us it started a while ago). They also discussed services that might be moved to, or from, the Crown Street site although such moves were already a fait acomplis, and the integrity of a Women’s Hospital seemed to be already lost.
We think it’s wrong that while the ICB follows a protocol to consult on service changes, the merging of the hospitals had no consultation whatsoever, and precious little discussion at the Liverpool Women’s Hospital Board. We were told at the engagement meetings, that merging hospitals does not need public consultation. This huge change was just ‘steamrollered’ through. Merging the Women’s is just the start. The intention is that the specialist hospitals in Liverpool, the Clatterbridge Centre, the Walton Centre and Broadgreen Heart and Chest, will be pulled into an even bigger merger. In contrast to LUHFT, the specialist hospitals have been funded nationally and do not share the financial crises facing LUHFT. It seems odd to us that such major reconfigurations are not considered to require public consultation, while (albeit cruel) changes to such things as celiac prescriptions do. At the ICB it was announced that they are going out to public consultation on whether prescriptions should still be available for gluten-free products for celiacs (A Gluten-free loaf can cost as much as £3.99.) We think this cut is terribly wrong for people already hard up, and struggling for enough food. Many celiacs don’t ask for prescriptions but the damage of this policy will hit the poorest hardest. The Celiac prescriptions cut is yet another cut amongst many – but surely, if this merits consultation, so must merging hospitals?).
Our campaign wants a well-staffed, well-funded Women’s Hospital on the Crown Street site. We want maternity to be funded and staffed well across the UK. We say enough of maternity scandals, enough of birth trauma, and enough of closures and cuts. We say this for all our mothers, daughters, sisters, friends, lovers, and babies. So many other countries do so much better than the UK in maternity and infant mortality. Once we were up with the best but austerity has damaged the service costing many of our babies’ and mothers’ lives, and women’s health.
We have 76,000 signatures on our petition to save Liverpool Women’s Hospital. People sent in many postcards opposing the idea of closure, or dispersal of services as set out in the engagement.
You can read more about the “engagement” process here from Greg Dropkin of Keep Our NHS Public.

We want to restore and repair the whole NHS, and to stop the relentless”Winter Crises”.
The NHS was founded to provide:
A national public service providing healthcare for all, free at the point of need, government-funded, publicly run, and publicly delivered, with well-qualified staff. For decades it worked very well, being declared the best health service in the world. Now it is seriously damaged and must be repaired.
The NHS came from decades of campaigning by working-class women, like the Cooperative Women’s Guild, and the Trade Unions, not from the rich and powerful. If we want to keep it we too fight for it.
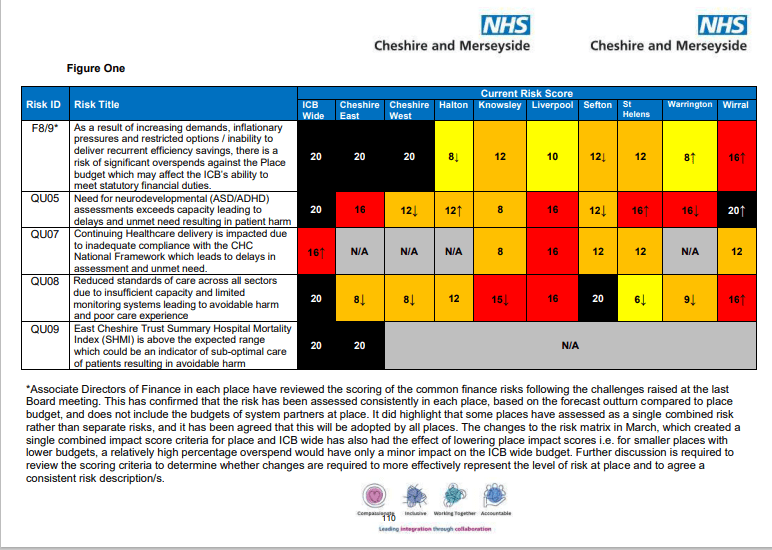
The NHS has seen reorganisation after reorganisation in favour of the American model, most recently the Integrated Care Model. The ICB for our area is called Merseyside and Cheshire ICB. This body controls the allocation of money to the hospitals and policy over cuts. Cheshire and Merseyside ICB, and other ICBs simply do not have enough money to function properly. They were conceived as part of a hospital closure project, to reduce the costs of the service and make it more acceptable to US health corporations take-overs. There are other hospital closure plans still going on, as well as the threat to Liverpool Women’s Hospital.
The ICB conducted an “engagement” with the public about the future of Liverpool Women’s Hospital. It was not well publicised but did include four in-person meetings for which they asked people to register. In all four meetings, their proposals were roundly rejected, but the attendance was small, very little effort was put into getting real engagement. We will write more about this in another post. None of the meetings were at a time suitable for working mothers to attend.
What you can do to help
Help with the campaign distribute leaflets and help getting the petition signed.
Raise it with your trade union, or other organisation
Tell your MP and councillor Liverpool Women’s Hospital must stay at Crown Street as a full women’s service run by experts in women’s health, in maternity and related services. Tell your MP that hospitals must cooperate not compete or merge.
Tell them that the winter crisis is unacceptable. Tell them that problems including finance, staffing, buildings and equipment must be sorted and the drain into private companies must stop.
Above all talk to people about this issue