Women and babies in Liverpool are entitled to the highest standard of healthcare. Our grandparents and great grandparents fought to found the NHS and left us this as their legacy. The NHS was a national service providing excellent healthcare, publicly provided and government funded. The new NHS did magnificent work for infant and maternal mortality.
In the last twenty years though, there have been years of cuts and privatisation in healthcare and years of poverty and subsequent ill health in Liverpool. A report to Liverpool city council this year said that, without change, “The life expectancy of women will fall by one year, and they will be in good health for 4.1 fewer years than they are currently.”
It is time to demand better.

We are campaigning to Save Liverpool Women’s Hospital and to restore and repair the NHS. We want to see improved funding and staffing and to see the whole NHS move back to its original model of a national public service, publicly provided, providing universal comprehensive and timely care for everyone free at the point of need and funded by Government. If you have not yet signed our petition please do so.
Healthcare staff have worked way beyond what should have been needed to keep some good services going. Every day people are grateful for their work, their kindness and humour but sheer human effort cannot compensate for inadequate funding and too few staff.
Liverpool Women’s Hospital provides some excellent services but it has some serious difficulties too.
The Liverpool Women’s Hospital board meeting on 9/05/2024 reported some excellent staff work, including improved methods of helping premature and very premature babies survive and thrive. It also reported the success of moving early pregnancy loss to its own area, a development much valued by the mothers involved. Previous meetings have seen patients reporting their experiences too. In April there was a very positive report from a patient about her experience of the care she received from the Rainbow Clinic as a previously bereaved mum. We have also seen excellent presentations about the pioneering work on endometriosis and menopause at different meetings. The Hospital website says Every day on average, 24 babies are born in Liverpool Women’s Maternity Unit and another three babies are born prematurely and cared for in our Neonatal Unit. Most of Liverpool’s babies are born at Liverpool Women’s Hospital and sick and tiny babies are cared for in the beautiful new NICU ( Neo Natal Intensive Care Unit)

The Liverpool Women’s Hospital is undertaking a major anti-racism drive to improve outcomes for patients and staff. We very much welcome this initiative. It is essential to save lives.
The core problem for Liverpool Women’s Hospital is under funding. This underfunding stems from the national underfunding of maternity as well as the general under funding of the NHS. This longterm underfunding has meant years of cuts. The NHS organisational changes from 2012 to create Trusts and Foundation Trusts also wasted many resources that should have gone to patient care.
Liverpool Women’s Hospital also has a long waiting list for cancer patients and waiting lists for gynaecology appointments. Some more staff have been appointed and hopefully the list will be dramatically reduced.These waits cost lives and health. The Chief executive reported that
“NHS England’s tiering process for cancer performance is designed to provide accountability and additional central support for trusts that are most at risk of missing national cancer targets. Trusts are categorised into tiers based on their performance, with Tier 1 being the most challenged and requiring the most support. Trusts may move between tiers based on their performance improvements or deteriorations.
In a letter received on 26 April 2024 from NHS England, it was confirmed that following a review of cancer performance, and in agreement with the regional team, the Trust will be in Tier 1 for Cancer from the week commencing 29 April 2024. The move to Tier 1 will involve regular meetings to discuss delivery progress and any required support from the relevant parts of NHS England.
Last year the hospital had a poor Care Quality Commission report for maternity and it has taken work to improve on this.New management is in place and they have plans to ensure that improvements are happening.

Our babies, our mothers, deserve much more.Every mother every baby treated at Liverpool women’s deserves the very best. Poverty from low wages, low benefits and poor housing is costing lives, and causing long term ill health. Inadequate health services are part of this.The Care Quality Commision report last year showed how much harm has been done by this underfunding and under staffing. The management must also be responsible for some of the damage mentioned in the Care Quality Commission reports.
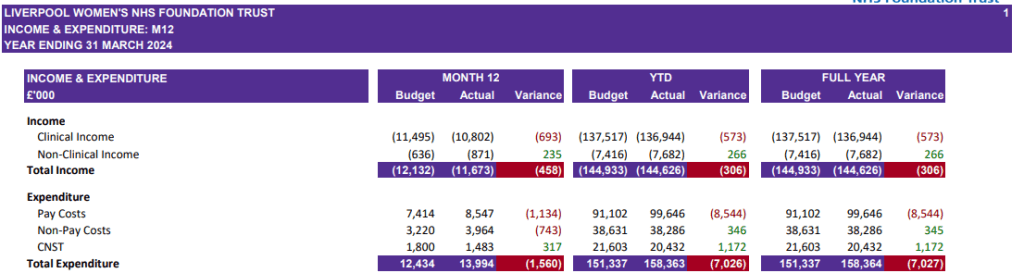
The funding issues at Liverpool Women’s means that to meet the current level of service it needs twenty five percent more funding. Money is spent very carefully but for basic safety to be met, that extra spending is essential. At present the required money is being spent and temporary support funding has been made available, by the ICB or national NHS. However this situation puts the hospital into whats called Level 3 of the National Oversight Framework which could bring in management decisions not based on the needs of staff and patients, as the government clamps down on public spending.
Many studies show that money spent on good healthcare repays for itself many times over. At birth this is especially so as bth injuries can last a lifetime.
Neither merging the hospital nor dispersing its services will change that fundamental financial situation. Only an improvement of maternity funding will make a real difference.
The underfunding of maternity leads to staff overwork and reduced services. Government safety figures for staffing are met but we say these safety figures are inadequate. The Government funding does not provide sufficient staff to deliver the kind of service patients and staff require. yet money is squandered on private companies and financial consultants.
There are national problems with maternity services described in many prestigious reports, as well as the Ockendon and Kirkup reports. No report has yet managed to shift the Government’s policies. We believe we need a huge campaign to win back the NHS.
A large part of Liverpool Women’s Hospital Maternity spend is on the maternity Incentive scheme, a government owned insurance system, run on a business model. Liverpool Women’s Hospital meets all the requirements of this scheme and so gets a refund from hospitals that do not meet all the safety requirements. This is an unbelievable situation..
Payouts from the fund are higher than the funding for maternity.If maternity were well funded fewer babies would be damaged and have to claim through the courts from this insurance fund.
In this crazy situation the hospital is still expected to make cuts (CIPs).

We have written before about how planned Cheshire and Merseyside ICB funding will not repair the situation patients experienced last winter. This poor experience was seen in many aspects, including A and E, care in corridors, access to GPs, access to NHS dentistry, and inadequate mental health provision. It will be worse next winter.
It was no surprise to hear there will be no new Hospital built in the next decade, nor does Liverpool Women’s require a new building. we believe that the new building idea was floated to make the idea of merging Liverpool Women’s Hospital into the big acute hospital more palatable. The existing building is less than thirty years old.However the drive to make fundamental changes remains, with merger or dispersal being the most likely recommendations. WE want to keep a distinct women’s hospital.
In the April Board meeting of Liverpool Women’s Hospital it was reported that work is in progress for major changes.
“the Women’s Hospital Services in Liverpool Programme. As part of the roadmap, the initial phase of the programme had been outlined, with an emphasis on the importance of openness, transparency, and continuous engagement with the public.
The development of a clinical case for change was scheduled for the spring and summer of 2024, with publication expected later in the same year. Feedback from this engagement phase, gathered during the winter of 2024/25, would then inform the approach to designing future services, with further development of potential options anticipated to commence in early 2025.” So the threats to Liverpool Women’s Hospital are still very real.
A meeting has been held with other Liverpool hospitals about the future for Liverpool Women’s Hospital and women’s health in the other hospitals in Liverpool.We have not yet been able to see which issues the other hospitals raised. Public consultation is promised this year.
No hospital can exist in a vacuum. Every hospital should be working in a mutually supportive system. The NHS was founded to be a national service, not a collection of competing hospitals. System working was damaged by the 2012 Act and the drive to privatisation. Cooperation and system working is required for the future of the other specialist hospitals in Liverpool, like the Heart and Chest and the Walton Centre.
Our campaign to Save Liverpool Women’s Hospital and to restore and repair the NHS has huge public support and is growing steadily.