The pandemic has been very hard on all of our families. We will touch on the impact of the pandemic and the many specific ways it has affected women. This includes women as patients, as healthcare workers, as the bereaved, as pregnant women, as mothers and carers, as workers on the front line, as disbled people, as young women, as students We have written earlier about the need to make the UK a safer place to be born and to give birth.

More than 124,000 people have died in the UK from Covid 19 since the pandemic began and 4.21 million have suffered from the disease. Internationally the death rate stands at 2.59 million whilst 11.7million are recorded as having suffered from the disease. Staff have developed better ways of treating the disease, and scientists have worked hard to produce vaccines.
The experience of dying in hospital cut off from family is frightening and heart breaking. Untimely and unnecessary death is dreadful. Even when death is inevitable the manner of our passing matters. Thankyou to all the staff have done their very best. The staff who have helped families say virtual good byes, holding i-pads and phones for the very ill patients. and those who have held people’s hands as they died, all are owed a huge debt of gratitude. We thank also those who have laid out the dead and pushed the trolleys to the mortuary. We mourn all our dead and recognize the suffering of many more. We offer condolences to friends and family of those who have died.

We send our heartfelt thanks to all the doctors, midwives, nurses, linked professions, healthcare assistants, cleaners and porters, and admin staff who are working through this pandemic, under paid, and under protected. Our NHS staff have stood like a bulwark against the pandemic, at great personal cost.
We mourn our many dead. We thank all the undertakers and the women of the churches who conducted funerals when no priests were available.
We send our best wishes to those still suffering from the virus, men and women, young and old, Black, Asian, Filipina and White. We send condolences to the very many bereaved, to those who have lost partners, children, brothers, sisters, parents, grandparents, family, friends and workmates.

Each of the men who have died are some mother’s son, many beloved partners, fathers, brothers, friends, neighbours, colleagues, work mates, neighbours. We fight for them too, for all in our communities.
We share the fury at the insulting pay deal offerred to nurses and the even worse one offerred to other NHS workers
We protest that it did not have to be this way. Effective, publicly owned, locally delivered, Find, Test, Track, Trace, and Support would have significantly limited the impact of this pandemic. Effective PPE for staff would have saved lives In the UK this responsibility rests squarely on the shoulders of the government. these essentials of public health are still not in place.
It is important to look at the impact of the pandemic, specifically on women. Although coronavirus physically affects men worse than women, women are being affected by the pandemic in multiple ways .We write as campaigners not academics, but only quote credible sources.
Women hold up half the sky but hold up more than three quarters of the NHS workforce. The NHS workforce are owed a huge debt of gratitude for their dedication, courage and sheer hard work. Sickness stress and death directly from Covid, and from the overwhelming workload have weighed heavily on the staff. We mourn the many NHS deaths.
We protest, however, that lack of decent PPE, equipment, of high quality building ventilation, the lack of truly reliable testing and ineffective tracing, and of the chronic and long term shortage of staff has led to many staff catching the virus in the hospital. We protest at attempts to gag staff from talking about these issues to the extent that we, the people, still do not know all of what happened.
WOMEN HOLD UP HALF THE SKY BUT HOLD UP SO MUCH MORE OF THE NHS
Our campaign shares the demand that the NHS be built back better after this pandemic. The pandemic must not be used as an example of best practice, nor an exemplar for the private sector as it is described in the White Paper The huge and expensive waste of money on Serco testing cost our people’s lives.
We salute the women who have worked to keep their communities fed and a deal saner than they would have been without the Mutual Aid. Providing food, school eqiupment, online support, phone calls and even passing chats whilst exercising has all helped. It has all knit our communities together and helped our mental and physical health
Even before the pandemic women’s life expectancy in good health was falling. Life expectancy in good health means how long a woman can expect to live in good health. Even though the government expects us to work until 68, but it is expected that by the age of 63.3 years on average women will no longer be in good health. “In 2017 to 2019, disability free life expectancy (DFLE) in the UK was 62.3 years for males and 61.0 years for females; there was a significant decrease of more than a year in DFLE since 2014 to 2016 for females, but no significant change was observed for males.” There are of course huge regional differences in this The wealthier you are the more likely to have an old age in good health. Austerity has taken a toll on women, and on the poorest people.
In the pandemic the infection rates of women and men seem to be similar, but women have lower death rate. Older people, women and men are more at risk. There are fewer older men than women so the death rate differences may reflect larger differences than at first appears. It is possible that estrogen may be protective factor. Underlying conditions have been used as an excuse for the deaths from Covid. Most women over 60 have underlying conditions and#s do many younger people.
We need to know how the pandemic has affected women, all women.
Many of our readers are users of Liverpool Women’s Hospital. The following two resources are worth using in pregnancy: https://your-healthy-pregnancy-tool.tommys.org/ and https://www.publichealth.hscni.net/publications/pregnancy-book-0. Also, this is the general advice from the NHS. Do not hesitate to ask for advice from your midwife during this pandemic, now more so than ever.
Advice on partners at the birth, now advises that partners be allowed at delivery and at key antenatal appointments.
You can find some information on pregnancy and the virus eight minutes into our meeting shown in this video
Fertility services have continued but have been limited by the pandemic. However, cuts and rationing had affected fertility services before the pandemic. That is another campaign we need to mount. Abortion services have continued with some disruption. The availability of medical abortion has been a usefule develpment in this pandemic. Please don’t hesitate to contact if you need help
Most pregnancies during the pandemic seem to have followed normal patterns. We could see no obvious problems (in a lay person’s reading) on Liverpool Women’s Hospital Board reports this month. We will continue to monitor this. The experience of birth has been more difficult especially for those women who were not allowed a partner at key appointments and the birth. Partners are now generally allowed. The latest research from Tommy’s found seven in ten pregnant women felt overwhelmed while pregnant, or during the early stages of motherhood, with 14 per cent saying they found it difficult throughout the duration. Stress does not help pregnancy and poorer women are the most vulnerable to stress. Worries about food, housing and heating are significant. The impact of stress in pregnancy can last for years.
The most recently published research from America indicates that Covid has been a risk for pregnant women.”Although data were initially unclear as to whether pregnant individuals are at increased risk of severe complications from COVID-19, a large study from the Centers for Disease Control and Prevention (CDC) provided data suggesting an increased risk. Among more than 450 000 symptomatic women of reproductive age with COVID-19 for whom pregnancy status was known, admission to an intensive care unit, invasive ventilation, extracorporeal membrane oxygenation, and death were all more likely among pregnant individuals than among nonpregnant women of reproductive age.3 Non-Hispanic Black individuals accounted for a disproportionate number of deaths. Symptoms in pregnant individuals (eg, cough, headache, muscle aches, and fever) were similar to those in nonpregnant women, although most symptoms were reported less often among pregnant individuals than nonpregnant women.3https://jamanetwork.com/journals/jama/fullarticle/2776447
Vaccine
The safety of the vaccines have not been specifically tested on preganat women but other vaccines have been shown to be safe, The general opinion appears to be that the risk of the disease is severe and best avoided, including possibly by using the vaccine. Please do check with your doctor
The Royal College of Obstetricians and Gynaecologists, the senior body on obstetrics posted these key points in March 2021
- The latest advice from the Joint Committee on Vaccination and Immunisation (JCVI) is that COVID-19 vaccines should be considered for pregnant women when their risk of exposure to the virus is high and cannot be avoided, or if the woman has underlying conditions that place her at a very high risk of complications of COVID-19.
- COVID-19 vaccines should only be considered for use in pregnancy when the potential benefits outweigh any potential risks for the woman and her baby.
- Women should discuss the benefits and risks of having the vaccine with their healthcare professional and reach a joint decision based on individual circumstances. (our emphasis)
- Breastfeeding women may be offered vaccination following consideration of their clinical need for immunisation against COVID-19.
- Women trying to become pregnant do not need to avoid pregnancy after vaccination and there is no evidence to suggest that COVID-19 vaccines will affect fertility.
- Having a COVID-19 vaccine will not remove the requirement for employers to carry out a risk assessment for pregnant employees, which should follow the rules set out in this government guidance.
Giving birth in the pandemic
Black and Asian women have worse outcomes in giving birth, even before the pandemic We don’t fully know the details of why, but as studies are published, we’ll share them. We have written about this before. Even with this awful discrepancy, the vast majority women, of every ethnicity, are safe. Some migrant women are subjected to high levels of charging for NHS services at 150% of cost. This has cost the lives of at least three women. We have long campaigned against any NHS charges.
“The MBRRACE-UK Confidential Enquiries into Maternal Deaths and Morbidity have highlighted before the disparities in outcomes for women from different ethnic minority groups. This year’s coronavirus pandemic has brought this disparity even more starkly to the fore, and we must not lose sight of the actions that are required to address systemic biases that impact on the care we provide for ethnic minority women…Pregnant women who are recent migrants, asylum seekers or refugees, or who have difficulty reading or speaking English, may not make full use of antenatal care services. This may be because of unfamiliarity with the health service, or because they find it hard to communicate with healthcare staff. Healthcare professionals should help support these women’s uptake of antenatal care services.”
Maternity Action reported in What price Motherhood.
Maternity care is undermined by charging, there will inevitably be poor health outcomes for mothers and babies. These are real people, not pawns in a game of political point scoring. It is difficult to see in the UK’s deliberately ‘hostile environment’ anything other than the inhumanity of bureaucracy flagged by Kafka. Charging guidance is deeply problematic, implementation is woeful and the research that informed these policies was flawed. Billing pregnant women at 150% of tariff cannot generate income from the destitute.
It is good to hear that the vast majority of pregnancies appear to have proceeded normally. However, during the pandemic some pregnant women did have virus issues.
Pregnant women who get ill with Covid. The NEJM reports that, internationally, ‘Although data on Covid-19–related risks to pregnant women and new-borns are limited, a recent study found that pregnant women with Covid-19 have 1.5 times the risk of being admitted to an intensive care unit (ICU) and 1.7 times the risk of requiring mechanical ventilation faced by non-pregnant women of childbearing age with Covid-19 but that pregnant women aren’t at increased risk for death.2Information on adverse pregnancy outcomes associated with Covid-19 is also limited. Intrauterine transmission of SARS-CoV-2 appears to occur rarely,3and no evidence has suggested an association between Covid-19 and birth defects; however, data suggest that preterm birth and admission to a neonatal ICU are common among infants born to SARS-CoV-2–infected women.’4
Women who must struggle to make ends meet are also at risk from the virus, from worse health and from problems in pregnancy.
Even without the pandemic post-natal mental illness has been a feature for some women. ‘It has been estimated that, across the UK, up to 1 in 5 women develop some form of mental health problem during their pregnancy or in the year after birth. The majority (81%) of women who responded to this survey experienced at least one perinatal mental health condition during or after their pregnancy.‘ (RCOG2017). Suicide is a risk. Mental health has been badly damged by austerity cuts and privatisation The Government need to provide better mental health support for women in pregnancy and for the year afterwards
Health visitors were diverted from their roles as support for new mums art the start of the pandemic, and have struggled to be returned An increase in perinatal mental illness and poverty was reported by 81% of health visitors surveyed, while 45% had experienced more families struggling with issues related to substance abuse.. We must insist that health visters numbers are increased immediately.
Women are more likely to work in the most affected sectors and more women have been furloughed.
According to the Institute for Fiscal Studies, by May 2020, mothers were 1.5 times more likely than fathers to have either lost their job or quit since March, and were more likely to have been furloughed. The Fawcett Society also found 35% of working mothers have lost work or hours due to a lack of childcare support during the pandemic.The Fawcett Society found that half of employed women from minority ethnic groups and 43% of employed women from White ethnic groups are worried about job or promotion prospects due to the pandemic. This compared with 35% of employed White men. The data does not state if White minority ethnic groups are included in the 43%.
Mothers, especially those with young children have been particularly impacted by the pandemic. Women from black and minority ethnic group have been very badly affected. The full reasons for this have yet to be understood but we know that racism, poverty, housing and frontline jobs, issues childcare are all part of the equation. We are working to understand this and have discussed it in our meetings. This article, though grim reading, gives some explanation at least inthe London context.
The TUC reported that 70% of mothers who applied for furlough were rejected. 80% ot those people who applied for financial support for self isolation were rejected. People have to choose between having the money to eat or self isolation. Consequently it has been in the poorest areas where take up of testing has been lowest, and where the virus has persisted longest. Heartbreakingly infections have spread through families many of whom have lost multiple members inflrcting incredible pain on the surviving family members. Liverpool has worked hard to get the testing and the vaccine out to the communities. We were pleased to see a win for the campaign ( of which we were part) to make sure everyone living in the UK had access to the vaccine.No one is safe until we are all safe. Thankfully the government has offerred a vaccine amnesty to all. Please let us know if there are problems with this. We still camapign for everyone to access the NHS free of charge a free of fear of the Home Office and the Hostile environment.
The lockdowns have had a disproportionate effect on women’s workload, especially on women who are heads of households .Managing on lower pay whilst facing higher bills for heating and food and wifi for education has bee na real strain. Women in paid employment who are able to work from home are more likely to see an increase in unpaid care work due to school closures and often caring for older dependents. Compared with men, women perform on average 3 times as much unpaid care and domestic work even though this is rarely classed as work (International Labour Organization 2018). The pressure of supervising home schooling and directly teaching children of different ages has been difficult for many. The problems of having the necessary tech and even paper and pencils has caused stress. For some families it has been a lovely time, one children will always remember.
Poverty has been shown to be appalling in this wealthy country. Mothers, we know, face the worst wages in the country. Our child care is a disgrace. Individual providers do their best but we need a universal well funded national system of child care, and shorter hours of work so parents can spend time with their children in the precious years when they are young. The UK comes 27th out of 48 countires in how well our children are provided for. This in a very wealthy country. Good childcare easy to afford would make life better for children and parents.
It is also a scandal that so many children do not have enough good food..UN data showed at least 8.4 million people in the UK struggle to afford the food they need.Official statistics from March 2019 showed that the number of children in absolute poverty had risen to 3.7 million, up by 200,000 in 12 months. Government support for children fell dramatically once austerity began. Poverty affects children even during pregnancy and affects outcomes at birth. Low wages for mothers is a major factor.

As well as being responsible for the bulk of domestic duties women are also providing most of the Covid-19 care in hospitals. Approximately 77% of health care workers are women and they also make up the majority of health service work such as cleaning, laundry, catering and admin work, so are more likely to be exposed to the virus. The women who keep our day to day life going, without whom all wheels stand still are often at greatest risk and lowest paid. According to a study by the think tank, Autonomy, and reported in The Guardian, there are about 3.2 million workers employed in the highest risk roles. Approximately 2.5 million are women and as many as one million of them will be among the lowest paid, many of them not entitled to statutory sick pay, putting them at greater risk as they choose between putting food on the table for their families or protecting their own health.
Mental health in the pandemic
The pandemic obviously increases the risk through stress and anxiety. The redeployment of health visitors away from new mums has not been helpful at all. We need more information on this. We would like to collaborate with those with experience of this and can share their insight.
The birth-rate has fallen in the pandemic, a situation seen at Liverpool Women’s Hospital and across the country.It is expected that the number of births in 2021 will fall further, for financial and social reasons.
Amanda Greavette

“In the first quarter (Jan. to Mar.) of 2020, there were 152,521 live births, 153,464 in Quarter 2 (Apr to June) and 158,452 in Quarter 3 (July to Sept). Or on average, approximately 52,000 live births per month).
Women have been impacted by reduced service from other health services affected by the pandemic. Breast Cancer Now estimates that a total of 986,000 women across the UK missed their mammograms due to breast screening programmes being paused.
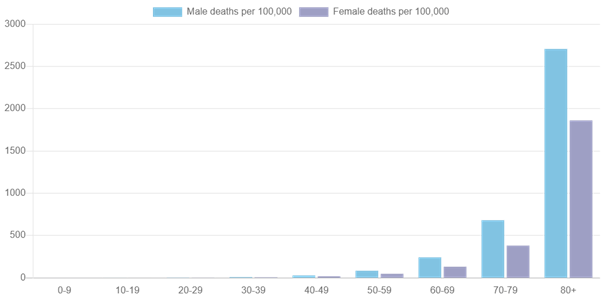
Men and women have different responses to the virus as the table below shows.
These two tables show cases of the virus and deaths from the virus by age and by sex.

Women are already suffering from poverty in the UK, whether from low pay, inadequate childcare, or from inadequate welfare payments, including the two-child limit on benefits.
We join the demand that support for people to isolate must be improved. We need much better sick pay for everyone. The virus can affect whole families because there is not room to isolate in small homes. We demand the kind of support made available in other countries. New York for example set up isolation hotels “The aim of the isolation hotel program was to provide a safe and supportive environment for individuals who are homeless, living in crowded or congregate housing, or whose family and/or landlords did not want them to return home out of fear of potential exposure to COVID-19. “https://www.liebertpub.com/doi/10.1089/HS.2020.0123
Domestic Violence
Lockdowns are putting women at higher risk of physical and sexual violence. The incidence of domestic violence in the UK has increased dramatically since the lockdown. Refuge, the UK’s largest domestic abuse charity, has reported a 700% increase in calls to its helpline in a single day (The Guardian). This at a time when the funding for women’s refuges has been drastically reduced. The Women’s Aid Annual Audit (28/01/20) showed that 64% of refuge referrals were declined last year. The number of bed spaces is now 30% below the number recommended by the Council of Europe. The key problems cited were all to do with inadequate funding. Only 5% of refuge vacancies listed last year could accommodate women with no recourse to public funds and less than a half had the capacity to accept women with more than two children.
Access to healthcare
Access to essential health services has decreased for the public during the pandemic. The consequences of reduced access to sexual and reproductive healthcare are particularly severe for some vulnerable women. The World Health Organisation has identified care during pregnancy and childbirth as a high priority essential service and all countries should prioritise to maintain this service (Geneva 2020). Women should have access to contraception, safe abortion and post abortion care to avoid unwanted pregnancies and sexually transmitted diseases.
Sexual and reproductive health care should be the right of all women. Women who use drugs, are sex workers or who live in poverty are at particular risk of contracting Covid-19, as are asylum seekers living in overcrowded accommodation and immigrants of insecure status. Yet they may lack access to healthcare due to fear of discrimination, deportation or health care charges.
When a pandemic strikes women must be consulted about the response. There are five basic demands published by the Women in Global Health Security Summit.
- Include women in global health security decision making structures and public discourse,
- Provide health workers, most of whom are women, with safe and decent working conditions,
- Recognize the value of women’s unpaid care work by including it in the formal labour market and redistributing unpaid family care equally,
- adopt a gender-sensitive approach to health security data collection/analysis and response management and to
- Adopt a gender-sensitive approach to health security data collection/analysis and response management
Marginalised and vulnerable women must be included in the response to the pandemic. Health care is a basic human right and should not depend on where you were born or the colour of your skin. We all deserve protection and to be treated with dignity. The cleaner needs PPE just as the doctor does.

The impact has been on wealth as well as on health. The Parliamentary subcommittee reported that “Evidence shows that the economic impact has been experienced differentially by women – and in many respects, more severely. Women are more likely to have primary responsibility for childcare. They are more likely to work in the service sector, and to be in insecure or zero hours work. And more likely to be more dependent on social security, and in insecure housing. They are over-represented in jobs which are not eligible for statutory sick pay.
We also know that the gendered impact may vary by ethnic group and that in some BAME communities, it is men who are most likely to work in shut-down sectors. We must consider what needs to change in the short and long term as the country emerges from the pandemic.”
Poverty is a crime committed on our children by the Government and by the lie of Austerity. Poverty kills children, and beyond childhood Fifteen years on Merseyrail takes fifteen years off your life”For half the people who have COPD, the condition is a reflection of childhood poverty.More than two in three children in some areas of the city of Liverpool are in poverty. Meanwhile the rich get quantitative easing with no means test, no demeaning questions about their sexual partners, no sanctions. The rich get huge amounts of money because the government says it will help the economy. We say putting food in kid’s bellies is much more important.
The Child Poverty Action Group reported before the pandemic “Even families with two parents currently working full time on the ‘national living wage’ are 11% (£49 per week) short of the income the public defines as an acceptable, no-frills living standard.
For lone parents, even a reasonably paid job (on median earnings) will leave them 15% (£56 per week) short of an adequate income because of the high cost of childcare. A lone parent working full-time on the ‘national living wage’ will be 20% (£74 per week) short of what they need to achieve a minimum standard of living.
Professor Ian Sinha, from Liverpool University and Alder Hey Hospital reported that “poverty hits children the hardest. Getting a job is not a solution. Most children in poverty have at least one working parent”.
“During childhood, we are especially vulnerable to the main determinants of health: living conditions, family income, employment, education, access to health services. The pandemic can be conceived as an additional systemic shock to these determinants. In the shorter term, with the focus squarely on adults with covid-19, child health and social care services are being side lined. These include acute services for life threatening illnesses, outpatient services for chronic conditions, child protection services guarding against abuse and neglect, and preventive services that support early years development, routine checks, and immunisations. Global modelling predicts a stark increase in child mortality as a result of diversion of care.6 As soon and as seamlessly as possible, we must restore these services to full, and greater, capacity.5”
Infants in more deprived areas are most likely to die. Listen to Ian Sinha here.
We must campaign to end child poverty and to improve the pay of mothers. Excellent family Allowances paid to the mother would really help.Wonderful people run food banks. However, the food available from food banks is not always nutritionally adequate. The pandemic is hitting children. Many children do not have access to food, let alone good, tasty food.
Pregnant women have been shown little respect by many employers in this pandemic. Maternity Action and Pregnant then screwed have reported in detail. At our “Let’s Get Rid of the Virus” meeting Roz from maternity action said how difficult it is to enforce our rights at work. Women in trade unions fared much better. because they were not alone in making requests . However the scale of responses to petitions aboout maternity leave has been such that parliament( as opposed to the government0 have had to respond
Women have joined trade unions and become more active in trade unions during the pandemic.TUC general secretary Frances O’Grady said: “…. figures show that union membership was growing before the coronavirus crisis hit. And we know that in the last few months, thousands of workers have been turning to unions to protect their jobs, defend their rights and keep their workplaces safe”
Young women are in the eye of the storm
The Young Woman’s Trust reports that
- an estimated 750,000 young women have had to go to work despite fears for their safety and protection against the virus.
- half of young women who are parents (51%) said they were unable to apply for or left a job because they could not cover childcare costs, up from a third of young women when the same question was asked last year
- a significant number of young women across England and Wales (43%) reported they had been offered a zero-hour contract (compared to 35% of young men) and
- over half of young women (57%) said they were worried about their mental health up from 51% last year. [2]
- Almost a quarter of young women with children said they had been discriminated against because of being pregnant, on maternity leave or returning to work after maternity leave (23%).
LGBT issues
A section of older lesbians and transwomen, who never married, socialise outside the home. This has been shut off during lockdown. Some have limited family support because of prejudice. Some younger LGBT people are stuck at home, sometimes with less than supportive families. The pro-tem closures of fertility services impact the LGBT community too, as they tend to be older approaching services for help in conception. Many more issues are discussed here.
Disabled people Among women, the risk of death involving coronavirus was 3.5 times greater for more-disabled women – defined as having their day-to-day activities “limited a lot” by their health – compared with non-disabled women.For less-disabled women, defined as having their day-to-day activities “limited a little”, the risk was two times greater.
Disabled people are 3 to 4 times more likely to die of Corona Virus. Disabled people account for 6 out of 10 deaths in the UK in 2020.Laws protecting disabled people were put at risk by Corona Virus legislation. 20% of men and 23% of women are disabled. The women’s budget group report that “Disabled Lone mothers lose out the most from tax and benefit changes since 2010; by 2021 they will lose 21% of their net income if they do not have a disabled child and 32 % if they do. A third of this loss is due to shift to UC.” During the pandemic disabled people have had services stripped away, services essential to their normal day to day lives. The pandemic has further disabled people. Similarly with disabled children. Pandemic legislation allowed these reduction of services. They must be restored
“COVID-19 death rates of people with learning disabilities have been between four and six times higher than for the general population.” The government reported that 451 per 100,000 people registered as having a learning disability died with COVID-19 between 21 March and 5 June, a death rate 4.1 times higher than the general population after adjusting for other factors such as age and sex.
But as not all deaths in people with learning difficulties are registered on these databases, researchers estimated the real rate may have been as high as 692 per 100,000, 6.3 times higher.
Deaths were also spread much more widely across the age spectrum among people with learning disabilities, with far greater mortality rates in younger adults, compared to the general population. The death rate for people aged 18 to 34 with learning disabilities was 30 times higher than the rate in the same age group without disabilities, researchers found.
People who need social care 1.4 million people who need social care do not have access to it even before the pandemic. “Social care has been a victim of unprecedented cuts to public services since 2010, which have seen local authorities reduce their spending on social care for older people in real terms by 17% despite rising demand“.
Women are having to work late into their 60s thanks to the pensions heist at the start of Austerity. Retiring at 68 women can expect limited years of good health, men even less. Forcing older people into work in this pandemic is cruel in the extreme.

The Independent reported in July 2019 that “Women’s pensions £100,000 less than men’s due to gender pay gap and childcare commitments.1.2 million women approaching retirement age have no savings at all.“
Just this week the government announced that many women had been under paid their pensions. other women working till 68to get a pension have been hard hit by the sheer weight of the manual work they have had to under take during the pandemic. We support reducingthe pension age for women down to 60 once again. The WASI women are correct. We would be quite happy for that to be available to men too.
Older women, after retirement ,provide a great deal of unpaid care within the family and community. Many organisations would be lost without them. Many care both for their elders and their grandchildren. The pandemic means that they have not been able to do this work, a loss for the community and to themselves as they have been much more shut in by the pandemic. Older women, especially grandparents, provide a great deal of childcare. Eighty percent of grandparents have provided childcare and many support the families financially as well. Grandparents very much value the chance to spend time with their grandchildren. The pandemic has broken many of these precious close family relationships. Hopefully, they will be rebuilt.
Older women have featured in care homes during the pandemic, others suffered by being cut off from family in the care homes, by being alone for exceptionally long periods and being cut off from family friends, cut off from their grandchildren and from the community, and from being out having fun with their friends, cut off from live music theatre, the cinema and more.
We will continue to look at how the pandemic affects women. Please send us any information or experiences you have.