Our next event is the ‘Human Billboard’ on International Women’s Day (March 8th). Please do come if you can. Commercial services can buy space on the many billboards around the city. We don’t have that money, so we thought it would be good to have supporters holding up banners on International Women’s Day, on the pavement outside Liverpool Women’s Hospital on the junction of Crown Street and Parliament Street. If you would like to come, make your own banner or hold one of the printed ones. Traditionally, International Women’s Day is celebrated with Bread and Roses, so feel free to bring flowers, cakes and dates. Some gentler music would be good too.
Then, on March 13th, everyone is invited to a citizen’s assembly called by Ian Byrne MP on the issue of the future of the Liverpool Women’s Hospital, at the Joseph Lappin Centre, Mill Lane, Old Swan, Liverpool. Again, the ICB will be invited, as will our campaign.
We await the next stage in the plans for Liverpool Women’s Hospital. Maternity services across the country have been severely damaged, and we campaign, with other Maternity campaigns, for a Maternity service fully staffed with properly qualified staff and much better outcomes for all mothers and babies. We are keeping a record of the reports on the problems in Maternity here. We are angry to see the greater risks to poor, Black, and Asian babies born in the NHS and the greater risk to poor, Black, and Asian mothers, and we make our call for better services and active anti-racism in their name, too.
We are forever grateful to the women and men who work in our healthcare, holding our lives and our bodies in their hands and working in unnecessarily tough conditions; a key demand of our campaign is to make the NHS a great place to work. Never a week goes by without our campaign getting messages saying how wonderful NHS staff have been that week and how tough the situations have been in the hospitals. We all deserve better. We supported the health workers’ picket lines and will continue that support in the future.
Only the very best for our babies, no ifs no buts.
Overworked staff cannot possibly provide the very best treatment. Birth trauma for mothers is a very real problem. Liverpool Women’s Hospital is one of very few Maternity units that has the approved level of staffing, but no one is fool enough to say that the current birth rate+ level is a desirable staffing level, it’s a minimum level. Our mothers and our babies deserve the very best. At present our service is not as good as other advanced European nations.
Gynaecology has also been badly damaged by years of cuts. This report was produced for Parliament. The situation is well-known and must be addressed.
Investing in healthcare has a huge return for the health and wealth of the country. It’s also a moral necessity. Paying millions to big companies and cronies is not necessary. Consultancies have bagged £600million just to advise on building new hospitals. £600 million would provide 1,000 more midwives for at least 6 years. The HSJ also reported this week that “Alan Milburn, the Department of Health and Social Care’s lead non-executive director, is a shareholder in and adviser to Bridgepoint HSJ. Practice Plus Group is owned by Bridgepoint Group, a FTSE 250 Index private equity company managing assets of €67bn (£55.5bn). In 2019 it set up PPG from the healthcare division of Care UK. Bridgepoint last year sold Care UK, whose main business is residential social care.“
The next stage in the current plans for the hospital, from the Integrated Care Board, should be reported to the ICB in March or April. The next meeting of the ICB is in Runcorn: 27 March 2025, 9.00 am to 12.30pm Location: The Events Hall, The Heath Business and Technical Park, Runcorn, WA7 4QX
The public can ask questions in the first half hour of the meeting, and listen to the rest of the meeting. We would have hoped that if the report from the engagement was to be reported, the meeting would have been held in Liverpool.
A major change of service in the NHS should have these stages:
Stage one is Public Engagement, and a report back to the ICB from the public engagement process. Technically, this stage was from October to November, but it seems to be carrying on. Then, the report produced at an estimated cost of £24,000 by a company that did not attend the public meetings nor the ICB board (to our knowledge) goes to the ICB. If the report is accepted more formal plans will be produced and go to formal public consultation.
We held a public meeting chaired by the local MP Kim Johnson, attended by almost 100 people. We will be posting extracts from that meeting in a different post. We invited the ICB to send a speaker to that meeting, but they declined. Had they attended, they would have spoken to more people than attended all the public engagement’s so-called public meetings combined.
We have distributed many leaflets and held stalls in the street.
Please also see our new post on Myth Busting about the situation with the plans for Liverpool Women’s Hospital.
Bread and Roses
This was our 2023 International women’s day poster, and still a favourite at at our stall.
The ICB, the lead body for the NHS in Cheshire and Merseyside, began a process towards significant change for Liverpool Women’s Hospital last year. It was formally announced in the autumn, and action got underway in October and November, with what they called an Engagement exercise. Their latest meeting was on January 30th. You can find all the papers we quote from the meeting here. There is also a long video.
Many people cannot understand how anyone could tamper with Liverpool Women’s Hospital. Some simply don’t believe that it is happening. We want to ensure that people can check what we post about the ICB against their own material. Quotes from their papers will be in blue.
There is no money for a significant improvement, let alone a new build, or for alteration of buildings in the existing hospitals. There is famously no room at the Royal, and given the winter crisis with trolley care at Aintree, no room there either. Any other site would be further away from the highest levels of intensive care than the current Liverpool Women’s Hospital site on Crown Street.
It is not possible to separate the fight for better Maternity care, better outcomes for babies, and better gynaecology and fertility care, from the overall privatisation, Americanisation, underfunding, understaffing and neglect of buildings in the NHS. Our campaign is part of a national fight back to Restore and Repair the NHS.
Leeds campaigners out in force.
What happened at the ICB meeting in January? During the “engagement” process in the autumn, the ICB presenters of their Case for Change stressed repeatedly that they wanted women’s services colocated in an acute general hospital, but that they did not yet have a plan as to how this would happen, or where our babies would be born. They insisted the Crown Street site did not meet national regulations. We have challenged this in detail here.
The issue of the future of Liverpool Women’s Hospital is managed by the ICB’s Women’s Hospital Services in Liverpool Committee.
TheSteps which are already taken towards their Case for Change.
Liverpool Women’s Hospital management was moved into a group with the Royal, Aintree, and Broadgreen, which was agreed upon at the ICB. How such a crucial change can happen without public consultation baffles us. We can find no legislation that permits this, but we will continue to look. There was legislation about the reorganisation of hospitals into Trusts. Trusts still legally exist, but they have delegated their powers over finance and staffing to the Group in Liverpool.
“Liverpool Clinical Services Review – Liverpool University Hospitals Foundation Trust and Liverpool Women’s FT come together as University Hospitals of Liverpool Group from November 1st. This will streamline decision-making and develop further collaboration opportunities in terms of service quality, access, workforce capacity and finance. Plans for other acute and specialist trusts to join a group structure, retaining their status as separate Trusts, are in development. “
Plans for the future of Liverpool Women’s Hospital are discussed at a subcommittee held in private, and their reports then come to the meeting held in public. At January’s meeting, it was reported that;
Phase 2 Programme Plan The next stage summary programme plan – from January – December 2025 – was presented to the Committee. The plan set out the timescales and milestones for agreeing the model of care, managing the options appraisal process and developing any business cases. The Committee approved the phase 2 programme plan.
and
Women’s services in Liverpool programme case for change approved by ICB board and formal public engagement started on October 15th. In parallel work will begin on the design phase and development of a clinical model at a Clinical Reference group meeting in December 2024. A Lived Experience Panel has been established to support the programme.
The (sub-committee) considered the following at its meeting in November 2024: Programme Update. This included: • Finalising the case for change and briefing councils and MPs prior to publication. • Planning and delivering the public engagement for the case for change. • Progress on delivering clinical improvements at LWFT. • Refreshing the counterfactual case. • Planning for the clinical engagement event in December.
“design phase and development of a clinical model” This phrase presumably is when they will decide where our babies will be born and where Gyny and the NICU will be based.
The report on the engagement meetings did not reflect the experience of many people who attended them. Before writin g this we checked with a dozen people who attended. Our campaign told people about these poorly advertised meetings, and we were the majority of the (few) people who attended. The in-person meetings were held during the day when people at work could not participate. There was only one evening meeting. We objected to how notes were kept at these meetings and that there was no recording. The overall response from the public was ‘NO!’ to their case for change. The report given at the ICB meeting said:
Communications and Engagement Update The Committee received feedback on the 6 week public engagement period which completed the day before the meeting.
The engagement process and products included face-to-face and online engagement events, a dedicated website, and a public facing version of the case for change (including an easy read version). Voluntary sector organisations were also commissioned to support the engagement with harder to reach groups and communities.
Feedback on the case for change was collected via a questionnaire (online, printed, and available in an easy-to-read format). This was also translated into 16 languages. An independent organisation, Hood and Woolf, has been commissioned to complete the analysis of the questionnaires; the Committee will receive the report of the analysis at its next meeting.
The engagement events proved to be challenging, with some individuals dominating the sessions. More resources are likely to be needed for effective engagement activities in the future to ensure all attendees can have a voice.
The plan for where the women’s services will go is not ready, and they don’t have the money for buildings or to fund significant change, but they intend to continue even in these circumstances.
Quotes about the finance for the Case for Change
“The C&M system is already financially challenged, and therefore the risk score reflects that new expenditure and investment may not be possible in the current financial climate; this is as much about the wider availability of public sector capital as the C&M situation“
and in more detail here
WSC3 – Failure to secure the required financial resources for the transformation of women’s hospital services in Liverpool, combined with revenue implications, will negatively impact on the successful delivery of proposals, currently rated as extreme (16). The C&M system is already financially challenged and therefore the risk score reflects that new expenditure and investment may not be possible in the current financial climate; this is as much about the wider availability of public sector capital as the C&M situation. A Finance and Estates Group is due to be established in January 2025 (as part of the emerging Programme governance and reporting arrangements). Further actions include baseline mapping to support the design phase and finance and estates modelling to support the options development – the latter action has a longer-term timescale of January – June 2025.
Date of next meeting: the Women’s Hospital Services in Liverpool Committee March 19th 2025
After the public meeting chaired by Kim Johnson MP on January 31st, with more people (around 100) in attendance than in the whole of the ICB “engagement” events in the autumn, we have been invited to a citizen’s assembly to be chaired by Ian Byrne MP for West Derby.
Other vital issues were discussed at the ICB meeting in January, including finance and the winter crisis. We will report on these in another blog post.
There is a lobby of parliament about the NHS. If you could go, please get in touch.
What does the Campaign to Save Liverpool Women’s Hospital want?
This is what we fight for!
Women having babies have the right to excellent antenatal care.
When giving birth, we need to keep our own agency, we need calm, and we need a good place to give birth, with well-rested, well-qualified staff available to be with us to help in a timely fashion.
Women and babies have a right to good restful care immediately after giving birth, with expert help in infant feeding and support with concerns. Mother and baby need speedy access to support in the early weeks and months in issues to do with physical and mental health.
That’s good Maternity care.
Next steps to Save Liverpool Women’s Hospital
We are planning a ‘Human Billboard’ – bring your own poster if you can -event outside Liverpool Women’s Hospital on March 8th at noon. Save the date.
We can do it!
We are collecting your stories about your experience with Liverpool Women’s Hospital. Please do get in touch.
We will be planning other public meetings around the city, holding stalls and leafletting events. We will continue to follow the meetings both at the ICB and at the Hospital Group.
Please invite us to any meetings you might be organising in the community, in your union or political party.
We need your help, and we need the money to pay for all of this. Please donate through Paypal or send cheques to Save Liverpool Women’s Hospital Campaign c/o News from Nowhere 96 Bold Street Liverpool l1 4HY
Response to the 2024 document: “Gynaecology and Maternity Hospital Services in Liverpool – Case for Change” Contributors Sheila Altés (Lead author), Felicity Dowling, Greg Dropkin, Rebecca Smythe.Thanks to Jim Hollinshead and Dave Pedder for their input.Published by Save Liverpool Women’s Hospital Campaign C/O News from Nowhere 96, Bold Street Liverpool L1 4HY (Postal address only) email savelwh@outlook.com
INTRODUCTION
The Women’s Hospital Services in Liverpool (WHSIL) programme was set up by NHS Cheshire and Merseyside Integrated Care Board (ICB) in January 2024, following a review of the way clinical services were organised across the Liverpool area (Liverpool Clinical Services Review January 2023). Its primary purpose was to: “Develop a clinically sustainable model of care for hospital-based maternity and gynaecology services that are delivered in Liverpool”
They concluded that the way hospital-based maternity and gynaecology services are currently organised did not provide women with the best possible care and experience. At a clinical engagement event in May 2024, a Clinical Reference Group was formed to review an earlier case for change. On the 9th of October 2024, this review was then presented to the ICB for approval at an Extraordinary Board Meeting – Women’s Services in Liverpool. The threat to re-locate Liverpool Women’s Hospital (LWH) surfaced once again.
BACKGROUND
Discussions to close LWH at its present site on Crown Street and re-locate to a smaller new building adjacent to one of the general hospitals in Liverpool began in 2015.
The emergence of austerity as the driving political ideology and with cutbacks in funding for the NHS meant that the Liverpool Clinical Commissioning Group (LCCG) had to close one of its hospitals. The Women’s Hospital, although less than 20 years old at the time and being massively underfunded, became a candidate. The then Chair of the LCCG announced, on a BBC Panorama programme, that Liverpool had too many hospitals and one had to close. The following day it was published in the Liverpool Echo that the chosen hospital was the Women’s Hospital (15 March 2015).
At that time the Five Year Forward View (later re-launched as the Long Term Plan) was published and the Naylor Review was commissioned.
Briefly, the Five Year Forward View was to make efficiency savings (cuts) by moving some hospital services to community care, which was deemed cheaper. Bed closures ensued and secondary care capacity reduced. However, resources were not invested into the community and social care services; this resulted in waiting lists for elective surgery increasing and longer stays in hospital for patients waiting for social care placements. Following the Health and Social Care Act (2012), the number of contracts awarded to private providers increased and lucrative contracts were awarded to private hospitals to carry out NHS-funded procedures in an attempt to bring down the waiting list (The King’s Fund 2021). This was a situation beneficial to private hospitals. They cherry-picked the most low risk uncomplicated procedures, leaving the more complex cases to the NHS. If complications occurred the NHS provided a safety net, as any patient needing critical care was transferred to an NHS facility. Compensation claims were also left for the NHS to pick up as they had outsourced the care to a private provider (Centre for Health and Public Interest 2014), The COVID pandemic exacerbated the waiting lists, this has led to an increase in the private health care insurance industry and an increase in patients paying for their own health care (British Medical Association 2024). But that was always the plan.
The Naylor Review, published in 2017, outlined how profits could be made from selling off NHS land and buildings. Its findings were in line with the requirements set out in the Sustainability and Transformation Plans (STPs) which were introduced in December 2015, to fast forward NHS England’s Five Year Forward View. Eventually, STPs evolved into what we have today, an Integrated Care System managed by an Integrated Care Board (ICB). This is a statutory body responsible for planning and funding NHS services over a large area. In this instance, the area is Cheshire and Merseyside, one of 42 such areas.
The Naylor Review, however, could only sell NHS land or close NHS buildings if there was a clinical reason for deeming them unsafe and “not fit for purpose”. And so began the construction of a clinical case for change at the Women’s and to re-locate it from its valuable Crown Street site.
The LCCG put forward several clinical arguments to strengthen their evidence for re-locating LWH:
Lack of adult critical care on–site
Patient transfers between hospitals
Inability to support women with complex health needs
Inadequate space for current neonatal facility
Unavailability of haematology/pathology services.
They then published a Pre-Consultation Business Case (PCBC, 2017) that set out several options for the re-location of LWH. Their preferred option was to build a new hospital at the site of the new Royal Hospital, and, connected to the new Royal by a link bridge. The plans were presented to the North West Clinical Senate for review. They declared it a suboptimal solution and only viable as a short-term solution because it was not co-located with children’s services. However, the Carillion debacle, and subsequent delay in completing the new Royal Hospital, the COVID pandemic, underfunding and reorganising of the NHS, and public opposition, forced these plans to be shelved until recently.
CLINICAL CASE FOR CHANGE 2024
There have been many improvements to enhance the quality of women’s hospital services in Liverpool. Many of these correspond to suggestions set out in The Alternative Clinical Case printed by Save Liverpool Women’s Hospital Campaign (Save Liverpool Women’s Hospital Campaign/Keep Our NHS Public Merseyside, 2017). Transfers between hospitals have been greatly reduced following the construction of a Community Diagnostic Centre. CT scans and MRI scans can now be carried out on-site. Plans to establish a 24/7 Blood Transfusion laboratory at the Women’s are underway, working in conjunction with Liverpool Clinical Laboratories. The care of pregnant women with complex needs is planned at many of the outpatient clinics at LWH. They are seen by a consultant obstetrician and a consultant of the relevant specialism to plan their care. A medical emergency team is being recruited. Joint multidisciplinary teams manage gynaecology patients with complex needs and there are joint operating lists on both the LWH and the Royal Hospital sites. A £10,000,000 development of gynaecology day cases is currently underway at the Crown Street site. The neonatal unit has been refurbished and extended to the cost of £15,000,000+. The hospital also has a new, state-of-the-art fetal medicine unit. Despite these and many other improvements at LWH, the ICB is intent on relocating LWH. Their Case for Change has identified 5 clinical risks which it states need to be resolved.
CLINICAL RISKS IDENTIFIED IN THE CASE FOR CHANGE
RISK 01
Acutely deteriorating women cannot be managed on site at Crown Street reliably which has resulted in adverse consequences and harm.
They state: This risk is caused by a lack of a range of services and specialist staff e.g. critical care, medical and surgical specialties, 24/7 blood transfusion labs.
Potential impacts include untimely transfers to other sites, delays to care and treatment, poorer outcomes, patient harm and death.
At present there is not an Intensive Care Unit (ICU) available at Crown Street, there is a high dependency unit (HDU) and staff working on the gynaecology HDU have undertaken training for critical care (LWH 2024a). The Cheshire and Merseyside Critical Care Network (CMCCN) has stated that providing an ICU at LWH would not meet national standards due to the “geographical and specialist nature of LWH”. At the public engagement meeting held on 20th November 2024 a member of the ICB agreed that an ICU at the Crown Street site would not be sustainable due to “low levels of activity”. In other words, so few women have needed intensive care that an ICU would not be feasible.
The Case for Change argues that LWH needs to be at the same site as an Intensive Care Unit. In the Case for Change review, they reference:
National standards for emergency care
Current clinical guidelines and recommendations
Core standards for Intensive Care Units.
They conclude that these recommendations state maternity and gynaecology need to be on the same site as an ICU. This is gross misrepresentation of these guidelines, they do not state that. The Core Standards for Intensive Care Units (2013) state that it is preferable to have an intensive care unit on site but units without such provision must have an arrangement with a nominated level 3 CCU and an agreed protocol for the stabilisation and safe transfer of patients to this unit when required. The RLUH is the nominated level 3 unit for LWH as part of local critical care arrangements and is situated approximately 1 mile away. The South East Clinical Senate’s recommendations are not mandatory. So, this ICB argument for moving LWH off the Crown Street site is un-evidenced. The Case for Change argument on this point is not supported by the South East Clinical Senate or by the Intensive Care Society (2013,2022).
ICB papers of the 9th October 2024 (page 7) state that 69 women were transferred from LWH needing critical care over a 4-year period, this equates to less than 2 patients a month. No comparative data was presented concerning adult transfers from other hospitals. The COVID pandemic occurred within that period, which no doubt affected these statistics. LWH is the recognised provider of high-risk maternity care and complex gynaecology procedures in Cheshire and Merseyside. It is inevitable that emergencies will occur and that transfer to a CCU will be needed. If services were moved to RLUH or the Aintree site women needing critical care would still be transferred, intra-hospital transfers need the same procedures as inter-hospital transfers. The women’s hospital in Birmingham is co-located with the acute hospital site and women needing critical care have to be transferred by ambulance. Inter-hospital transfers of critically ill adults happen frequently. NHS England data from the 2019/2020 year demonstrated that there were between 20,000 and 25,000 adult critical care transfers performed and the numbers may be higher (Adult Critical Care Transfer Service 2024).
ACUTELY DETERIORATING WOMEN
It has been noted that, sick pregnant or recently pregnant woman can present to health professionals in any location; emergency departments, walk-in centres, medical or surgical wards or in the community and general practice. Enhanced Maternal Care Guidelines were published in 2018. They summarise recommendations for the care of pregnant or recently pregnant women who become acutely or chronically ill. They state that early recognition and management is essential and a system to do so to be in place. The Maternity Early Observation Warning System (MEOWS) is a system that is used by clinicians at LWH to alert them to any deterioration. According to LWH website (LWH 2024b) there is a broad range of services for enhanced maternal care at LWH. They include: enhanced midwives, a perinatal mental health team and specialist antenatal clinics. A Medical Emergency Care Team is being recruited to enable optimal care and transfers if necessary. A 24/7 on site consultant obstetrician is planned. The Women’s has been selected as a Maternal Medicine Centre (MMC), one of 3 in the North West. This will provide regional care for safer outcomes and better birth experiences (Liverpool Women’s Maternal Health Centre July 2022 (LWH 2024b)).
The ICB has focused on a minority of women who have needed to transfer to ICU but have failed to take into account the 50,000-plus patients who use services at LWH each year
RISK 02
When presenting at other acute sites (e.g. A&E), being taken to other acute sites by ambulance or being treated for conditions unrelated to their pregnancy or gynaecological conditions on other sites, they do not receive the holistic care they need.
They state that there is a lack of women’s services and specialist staff at other sites in Liverpool. They go on to say that the potential impacts are the same as for risk 1 i.e. untimely transfer to other sites, delays to care and treatment, poorer outcomes and death.
It is difficult to see how relocation would solve this. If LWH were re-located to the RLUH, women are still likely to turn up at the Aintree site and vice versa. Is the ICB envisaging maternity and gynaecology services at both sites? Neither the Royal nor Aintree provide all services on-site. This dispersal of services would not fit with the ethos of a specialist hospital for women and that would be a gender inequality as women’s health differs from that of men in many unique ways. It is influenced, not just by biology but also conditions such as poverty, employment and family responsibilities. Women’s reproductive and sexual health has a distinct difference compared with men’s health. Cardiovascular disease, common to men and women, can lead to pre-eclampsia in a pregnant woman. Sexually transmitted infections can cause such outcomes as stillbirth or neonatal death. There is a long history of women with health issues being misdiagnosed or dismissed by doctors (Dusenbery 2018). Breathlessness and chest pain are often labelled as anxiety and not a symptom of heart disease (Hatherley 2022). Severe pain, heavy bleeding and irregular cycles are often dismissed as “just having a period” and that women should just “put up with it” (Wellbeing of Women 2024). This could lead to women receiving poor treatment and misdiagnosis (Cleghorn 2021) A study by Manchester Metropolitan University (2024) found that health care providers poorly understood endometriosis, the study found that it takes an average of 7.5 years to get a diagnosis of endometriosis. There is a lack of research in how medication can affect women, they are more likely to have side effects as the outcomes of clinical trials usually focus on men as the default patient (Modi, N 2022). Female cells respond differently from male cells and hormonal changes in women can affect how drugs are metabolised, yet women are often marginalised in clinical trials (Sundari 2020). Other issues impacting on women’s health include unplanned pregnancy, non-consensual sexual activity, domestic violence and female genital mutilation.
These issues are well known to the specialist staff at LWH. At the meeting held on the 9th October, it was pointed out by a member of the public that if relocation of the Women’s took place, to no matter which site, there would only be one A&E department at that site and pregnant women and women with gynaecological problems would be taken there. He also pointed out that the Board’s own data state that 120 pregnant women attended the emergency department at either the Royal or Aintree site. This does not necessarily mean that they were transferred from the Women’s. It means that an emergency situation occurred while these women, who happened to be pregnant, were going about their everyday business, so of course they went to the nearest emergency department. This would happen no matter where the Women’s was located. The situation at the Royal A&E department in particular, is dire, with long waiting times and corridor care, whereas, at the Crown Street site there is a designated Emergency Department (ED) with clinicians who have a better understanding of women’s health than those at a general A&E department and much shorter waiting times. LWH provides an outreach midwife service to support pregnant women who are at other trusts in the city.
The majority of these women will have booked their ante-natal or post-natal care at LWH. The table on page 86 of the Board papers shows that in 2023 they supported a total of 35 patients. Conversations with medical staff at Royal Liverpool Hospital state that if a pregnant woman presents there and they have concerns, they immediately consult with the outreach team and if a midwife is needed they present promptly.
The data included in the clinical case for change report (NHS Cheshire and Merseyside Integrated Care Board, 2024) that in a 4 year period (2018-2022) there were 19 serious clinical incidents in gynaecology and maternity. Isolation from other hospital services was cited as a major causal factor but not a root cause. These are still very small numbers and do not take into account the effect of the COVID pandemic. Further data state that 148 clinical incidents, not individual patients (our edit), occurred in a 21 month period and were caused in full or in part by the Women’s being on an “isolated site”. They do not give any indication of their outcomes.
The figures showing the number of critical care transfers on page 55 of the Case for Change (lbid.) show that in 2018 there were only 8 transfers and 12 in 2022, the highest figures occurred between 2019 and 2021, during the Covid pandemic. Data presented on page 84 of the case for change show that over the last 6 years, 39 patients were transferred to RLUH from LWH that were defined by ambulance services as category 1, and there were 31 transfers to LWH from RLUH in the same category. Category 1 is a life-threatening, time-critical event needing immediate intervention. In category 2, defined as emergency, needing either on-site intervention or urgent transport there were 558 and category 3 which is an urgent problem but not life-threatening, there were 90. While some of these figures may sound alarming, they were over a 6 year period including a global pandemic, and compared with the estimated 25,000 transfers of critically ill adults annually in the UK, they are in reality very small numbers. The categories cited are relevant to the ambulance service. Critical care is not the same as emergency care. The main difference is that emergency care focuses on treating life-threatening injuries and medical conditions needing immediate treatment at the scene. Critical care focuses on the very ill patients needing round-the-clock attention from a specialised team of health professionals. Patients needing transfer from LWH to a critical care unit are stabilised before transfer. There are protocols in place to optimise the safe transfer of women and babies. Ambulance transfers between Aintree and LWH; there were 10 in category 1, 42 in category 2 and none in category 3, a total of 52. This was over a 6-year period.
In view of the evidence that women are marginalised in healthcare, it is ludicrous that the ICB is considering re-locating a hospital dedicated to women’s reproductive health to an acute general hospital where they are less likely to receive specialist care.
RISK 03
Failure to meet service specifications and clinical quality standards in the medium term could result in a loss of some women’s services from Liverpool.
They state that this risk is caused by an inability to meet key clinical co-dependencies due to lack of co-location of women’s hospital services with other adult hospital services.
The risk would disproportionately impact women and families from more deprived backgrounds who may not have the resources to travel outside the area.
All service specifications could not be met by co-location with either the Royal or Aintree. As the Board papers state, both acute sites cannot meet clinical standards and specifications either (page 88). Even if women’s services were to be re-located at both sites, specifications and co-dependencies would not be met as women’s and children’s services would not be co-located. This is unlikely to happen, given the considerable financial investment in the new RLUH and Alder Hey Children’s Hospital.
No hospital can provide for every eventuality. The Board papers state that some women have to travel to Manchester for their treatment. This implies that the treatment they need is not available at the acute sites in Liverpool, how will re-locating LWH change this? People are transferred out of their area for more specialised treatment every day. Certain procedures for some cancers are only available at the Christie Hospital in Manchester, ECMO( extracorporeal membrane oxygenation) is only available at 5 centres in the UK, cyber knife radiotherapy is available for NHS patients at 3 centres, and thrombectomies at 24 centres. Using transfers for complex procedures as an excuse for re-locating LWH is unreasonable.
LWH is a centre of excellence specialising in the health of women and babies, not only in Merseyside but in the wider North West region, parts of North Wales and the Isle of Man. It is the largest single-site maternity hospital in the UK and staffed by dedicated teams specialising in, obstetrics, gynaecology, anaesthesia, genetics, fertility, nursing and midwifery as well as researchers and educators. Many of these are internationally renowned consultants with a wide range of special interests including; hypertension, diabetes, maternal and fetal medicine, gynaecological oncology, pelvic floor surgery, palliative care, haematology, urogynaecology, polycystic ovarian syndrome and many more (LWH 2024c).
In March 2023, as part of the NHS commitment to halve the maternal mortality rate by 2025, specialist medical care centres for women during pregnancy were established. LWH, as a centre of excellence, was selected as one of 3 such centres in the North West, the other 2 being at Manchester Royal Infirmary and Royal Preston Hospital. The aim was for pregnant women with serious medical problems to have access to specialist treatment at these centres. In all there are 17 such centres across the country and networks linked to these centres will ensure that access to expert maternal medicine care is available to all women (LWH 2024b).
These centres will be able to provide treatment and procedures that are safe in pregnancy. Following an initial assessment, if their condition is well managed they will be given a management plan to continue at home with support from their local maternity team. The most serious cases will be closely monitored with specialist treatment by the centre. As well as all of these services, LWH is currently working towards being a designated provider of complex termination of pregnancy, endometriosis, placenta accreta and fetal therapies, in partnership with Alder Hey (Case for Change, page 87).
It is difficult to believe that services could be withdrawn from such a prestigious, regional centre of excellence that has been selected as a Maternal Medicine Centre. NHS England would have been aware of the configuration of services before its selection.
RISK 04
Recruitment and retention difficulties in key clinical specialities are exacerbated by the current configuration of adult and women’s services in Liverpool.
They state: this is caused by the inability to provide comprehensive onsite multi- disciplinary team (MDT) working and training on acute sites. MDT training and working is emphasised in current clinical practice, however this is hard to achieve in women’s hospital services in Liverpool. Roles in Liverpool may seem less attractive because of the current service configuration. Clinicians may feel exposed and/or unable to perform their duties without outside support from the wider MDT.
The potential impact of this risk is that vacancies may persist. Services could become increasingly fragile and difficult to deliver. There would be a negative impact on existing staff leading to increasing turnover and recruitment difficulties.
Recruitment and retention of staff is a national crisis in the NHS as a whole and not just in maternity services. The Royal College of Midwives estimates that there is a shortage of around 2,500 full-time midwives working in the NHS (January 2024).
A search of job vacancies at the Women’s in October 2024, showed a vacancy for one staff nurse on the Hewitt Suite and one midwife for fetal medicine and one genomic practitioner, the rest appeared to be administrative vacancies. At the Board meeting of 9th October 2024, we were assured that LWH had its full complement of midwives according to the calculations of Birthrate-Plus. This is a system to calculate the required number of midwives to meet the needs of women throughout pregnancy, labour and the post-natal period both in hospital and in the community setting. This system has been in place for a number of years and although some believe it to be reliable, others differ in opinion as there are no comparable studies of other methods (Griffiths et al 2024). At LWH there have been a number of newly qualified midwives recruited, and although there is a preceptorship pathway in place to support them, the reduction in older more experienced midwives, due to retirement, will have a negative effect on their development of skills and knowledge.
Board papers suggest that multidisciplinary team (MDT) training and working is not provided at the Women’s. This is untrue. There is a multidisciplinary team of specialists who meet regularly to plan the care of pregnant women with complex needs. Now that the Women’s has been selected as an MMC, the MDT will include specialists from all over the region. The collective knowledge can only benefit patients and staff alike
The Women’s has always been innovative in conducting research to improve women’s health. The Midwifery Research Unit was the first of its kind in the country and conducted a wide variety of research in childbirth. LWH protocols are used in maternity units across the country and are a point of reference for setting protocols in many such units.
As a teaching hospital, LWH is a centre of excellence in the provision of undergraduate and postgraduate medical education and training. According to its own website LWH has “an extremely active multidisciplinary research programme that includes research into maternity studies, gynaecology studies, fertility studies, genetics, oncology and neonatal studies” (LWH 2024d).
The wide range of services available at LWH, makes it ideal to advance research and conduct large-scale clinical trials.
That its location, one mile from an acute hospital site, makes it difficult to recruit and retain staff is hard to believe in view of the fact that it has its full complement of midwives and clinical staff, many of whom have been there for several years. What could have a negative impact on recruitment is more likely to be the 9-year threat to reconfigure services at the Women’s and the lack of certainty of its future.
RISK 05
Women receiving care from women’s hospital services, their families and the staff delivering care, may be more at risk of psychological harm due to the current configuration of services.
They state: There is a risk that pre-existing levels of psychological harm and stress could be exacerbated for women, their families and staff, by the suboptimal way services are currently organised.
There is evidence that 4-5% of women develop post-traumatic stress disorder (PTSD) every year after giving birth and high numbers of staff working in gynaecology and maternity services report work-related trauma and symptoms of PTSD.
Delays and workarounds in care can have a negative impact on clinical outcomes, quality of care and patient experience which could create or compound psychological trauma for women, their families and staff.
For the last 14 years NHS staff have been underpaid, overworked and undervalued, conditions that were exacerbated by the pandemic and still continue. The Ockenden review highlighted these issues up and down the country, so psychological problems are not exclusive to the Women’s Hospital.
In a time of increased misogyny, violence towards women and austerity policies that disproportionately affect women, LWH is seen by all women of all ethnicities, who use the services, as a safe place for women.
Liverpool Women’s Hospital is situated in a quiet, landscaped and safe environment. Within the hospital grounds, there is a memorial garden that offers a private space for bereaved families. Another garden was opened in 2016, “The Garden of Hope and Serenity”.
“The idea for this garden came from our gynaecology nursing team who recognised that women and families visiting our Emergency Department at times would benefit from an area away from but adjacent to the department to have time to reflect on conversations with staff and have space and an area of calm to process their thoughts and feelings” (Allison Edis, Deputy Director of Nursing and Midwifery, in 2016, cited in Liverpool Women’s Hospital. 2024e).
There is a wealth of literature that confirms the importance of trees and gardens for patient recovery. A much-cited study by environmental psychologist Roger Ulrich was the first to use the standards of modern medical research to demonstrate that gazing at a garden can sometimes speed healing from surgery, infections and other ailments. It has been proven that just looking at views dominated by trees, flowers or water for a few minutes can reduce levels of anxiety, anger, stress and pain. This can allow other treatments to help healing and induce relaxation that can be measured in physiological changes in blood pressure, muscle tension brain and heart activity (Ulrich 1984).
Studies have shown that loud sounds, disrupted sleep and other stressors can have serious physical consequences and hamper recovery (Ulrich 1991).
Henry Marsh, the celebrated neurosurgeon has stated:
“…these big hospitals are horrible places really, the very last thing you get in an English hospital is peace, rest or quiet which are the very things you need the most”. He goes on to say that the garden he created at St. George’s Hospital “is probably the thing I am most proud of” (The Observer, 2017).
Although the Women’s is situated in a fairly central location it is protected from the sounds and pollution of traffic. There is substantial evidence on the adverse effects of air pollution on different pregnancy outcomes and infant health, including lower birth weight, neonatal jaundice, fetal death, maternal anaemia and other adverse outcomes (Rani and Dhok, 2023).
In the face of all the evidence of the harmful effects of air traffic pollutants on neonates, it is inconceivable that the environmental effects of relocating LWH to either of the acute hospital sites, both situated in the most traffic-dense areas of the city, have not been considered.
Summary
The Case for Change presented to the ICB on the 9th of October 2024 is weak and relies on data gathered before the many improvements at LWH and listed on pages 43 and 44.
The most contentious of the risks that they present focuses on transfers for critical care. On page 7, they state that between 2018 – 2022 there were 69 transfers for critical care, that is, 17 a year. They don’t mention that there was a pandemic during this period, nor do they give figures of transfers between RLH and AUH over the same period (no one is suggesting moving AUH to RUH).
Page 7-8 says that there were 73 serious clinical incidents in gynaecology and maternity services in the period of 2018 -2022. In a clinical review of these incidents, isolation of women’s services from other hospital services was found to be a causal factor in 19 of these incidents and 7 of the 19 involved a transfer for critical care. That is 2 transfers a year. How does it make clinical or financial sense to move a hospital to deal with 2 transfers a year?
Page 8 states there are around 220 ambulance transfers between LWH and either the Royal Liverpool or Aintree hospitals a year, stating that Category 1 or Category 2 made up around half of these transfers. They do not say how many were Category 1 or how many adverse effects there were. They do not make clear if any of these transfers were repatriation transfers.
Page 8 also refers to 148 clinical incidents from July 2022 to March 2024 caused in full or part by women’s services being provided on an isolated site. They do not state if these incidents were in a red, amber or green category. Previous clinical incidents cited in Board papers described one clinical incident as due to there not being a fridge to store breast milk. They do not state if any of these incidents involved transfers.
Page 8 also states that women needing critical care transfer or presenting in Emergency Departments whilst pregnant are more likely to be from ethnic minority groups and socially deprived backgrounds. Where is the evidence that they make up the number of transfers from LWH for critical care?
Page 107 states that the organisation of gynaecology and maternity services in Liverpool has created a significant gender inequality. How is the inequality caused by the organisation and would reorganisation decrease or increase the inequality? They say that this puts women using these services at a disadvantage when compared with people using these services in other parts of the country and men and women using services at other hospitals in Liverpool. Where is the evidence to support this? They go on to state that the demographic profile of women using these services compounds and increases those disadvantages. Where is the evidence? The demographic profile would remain the same if LWH relocated. Where is the evidence that BAME and deprived communities have better treatment at the Royal and Aintree than at LWH?
Page 63 on maternal mortality at LWH is in line with national rates. But LWH intake has more BAME and more deprivation. These factors increase maternal mortality so LWH achieving the national rate means it is doing well. On page 8 paragraph 2.18 they strengthen this argument by reference to MBRACE re impact of deprivation, Black, Asian, severe and multiple deprivation.
Page 94 section 4.4 states that staff at LWH are exposed to events that can trigger the development of Post Traumatic Stress Disorder (PTSD). All health care staff working in the acute setting are exposed to traumatic events. How can relocation prevent this? There are no comparative data from other Trusts about levels of referrals to a trauma-based psychology service. Other factors causing stress among staff could be bullying, overwork, pay, and not being listened to. In LWH Board papers (October 2024), a staff survey showed that 49% of staff feeling negative about their work stated they felt overworked. How is psychological harm to families and patients measured? What about the psychological harm from moving out of L8 and the negative impact on BAME and deprived communities? L8 is home to many BAME women who are reluctant to use public transport due to racial harassment. Relocation to either of the 2 acute sites would put them at risk of harm, both physical and psychological if they were forced to travel on public transport. Has this been addressed?
Page 98 quotes the Royal College of Midwives Maternity Services Report, on a 78% increase in birth to mothers over the age of 40, this in the years 2001 to 2014. The Case for Change does not state any adverse effects, only a need for an increase of resources. Older women may have more risks but this does not equate to high risks. These women will be monitored more closely but if the mother-to-be is healthy then pregnancy will be straightforward (Knight, M.2016). Those with more complex needs will be monitored in the same way as other expectant women, regardless of age, in the many specialised clinics at the Women’s. Re-location will not affect this.
Conclusion
The Case for Change presented to the ICB on 9th October, did not provide any proposals or solutions, it focused on adult maternity and gynaecology hospital services and did not include neonatology. (newborn babies)
It held public engagement sessions to gain feedback from the community. How can a public engagement on such an important topic be held without specifying what the change would be?
How are the public meant to decide on a change without knowing the alternatives?
It is also inconceivable to discuss a change in maternity services without including neonatology. What are the consequences of change for the babies?
When changes to maternity and gynaecology services were first discussed in 2015 the conclusion of LCCG was to build a new hospital adjacent to the new Royal Hospital and connected by a link bridge. This did not materialise. CCGs were closed down following the Health and Care Act of 2022 and ICSs were established and managed by ICBs.The Cheshire and Merseyside ICB has repeatedly stated that there are no funds available to build a new hospital unless it applies the previous government’s definition of a new hospital which could be:
A whole new hospital on a new or current site
A major new clinical building or wing of an existing building
A major refurbishment and alteration of an existing hospital.
As the ICB is focusing on a change in the delivery of maternity and gynaecology hospital services, the reality could be that they are delivered in a wing of one of the existing acute hospitals. The site of the new Royal does not have sufficient space to accommodate the range of services available at LWH at Crown Street, unless it moves some existing services from its current site. The land where the old hospital stood is earmarked for the development of an academic health sciences campus.
Similarly, at Aintree Hospital space is not available unless it moves some services to other areas. Neither solution would provide all services that their case for change deems necessary to comply with standards of co-location of services. They could even be considering 2 small units, one at each site. This would disperse services and the whole ethos of a special hospital for women would be lost. Both acute hospitals are in areas of heavy traffic and parking facilities are inadequate at both sites.
The Case for Change focuses on the safety of services at the Crown Street site. A Care and Quality Commission (CQC) review carried out on 15th January 2024 cited some safety concerns in maternity mostly to do with staffing levels, updates in training, record keeping and staff feeling undervalued, and not respected or supported by management. None of the issues mentioned the site being isolated. Improvements were made and a subsequent unannounced inspection by the CCG gave a rating of good. The recent maternity scandals have all been in co-located hospitals. The maternity services are under-funded and this, with undervalued and underpaid staff have contributed to the tragic events reported across the country together with the non-prioritisation of women in general hospitals.
The Cheshire and Merseyside ICB has a deficit of £150 million. Closing hospitals and reducing bed numbers is a standard response to financial problems imposed by government. Is the Women’s the first of Liverpool’s specialist hospitals to be under threat? We have been told for many years that Liverpool has too many hospitals. The people of Merseyside and Cheshire are fortunate to have so many centres of excellence in their area. This should be a cause of celebration not looked upon as detrimental.
We can only speculate on the ICBs intentions in the absence of any proposals. Are they moving towards the centralisation of services as has been the recent trend? An evaluation of centralising hospital services in Denmark, found that it did not always improve the quality of care (Christiansen, 2012
All maternity units nationally are under-funded, the maternity tariff is inadequate as is Birthrate- plus as a tool to calculate the number of staff needed to meet clinical needs. Staff continue to feel overworked. To improve maternity and gynaecology services nationally, bursaries should be provided for nursing and midwifery students and university programmes for midwifery should be better staffed and funded. Changes need to be made to doctors’ training so they gain more general experience and not concentrate on specialities. Enhanced training for all healthcare professionals in managing women’s health issues and conditions should be provided. Re-location will not solve this. In Cheshire and Merseyside, adequate funding, improvements to workforce training issues, providing emergency obstetrics and gynaecology services at A&E departments at the acute hospitals will all improve quality of care of women in the area. No closure, no privatisation, no cuts, no merger, reorganise the funding structures not the hospital. Our babies, mothers and sick women deserve the very best. These are the changes needed, not the re-location of LWH.
In the event of moving women’s health services from Crown Street, what will become of the building? The ICB has repeatedly stated that it will be used for NHS services: for example, they have considered the Crown Street site being used for out- patients and day case procedures. The question is who will provide these services when they are put out for tender? Will we see Spire Hospital providing NHS funded elective surgery or Spa Medica providing ophthalmology services? That would not sit well with the people of Liverpool.
We remind the ICB once again of the significant investment of the NHS in LWH as a considered effort by the then Dean of Liverpool, to invest in the L8 area through his Project Rosemary following the Toxteth uprising. LWH is a much-loved hospital dedicated to the care of the women and babies of Liverpool and surrounding areas and should remain so.
Save Liverpool Women’s Hospital Campaign/Keep Our NHS Public Merseyside (2017) Response to the CCG’s Review of Women’s and Neonatal Services regarding the clinical case for change Available at: https://www.labournet.net/other/1612/clinical1.pdf (Last Accessed 14/12/2024)
Sundari, R. (2020) Making pharmaceutical research and regulation work for women British Medical Journal (Online) Vol.371, p1-5 Available at: https://www.jstor.org/stable/27239697
Please help the struggle to restore the NHS. ‘People power’ can change government policies, and the current neoliberal, pro-privatisation, pro-business policies are at the root of the problems in our hospitals, in our GP practices and in social care. Write to your MPs, write to your councillors, raise it in your union branch, make the NHS the talk of the town, of the streets, of the communities, of the workforces.
Look out for the public meeting that will be held.
Stay safe and keep warm. Put the heating on.
Restore the NHS as a fully public service, funded and staffed for all our mothers, daughters, sisters, friends, lovers, and every baby.
Restore the NHS as a fully public service, funded and staffed for all people.
We are the Save Liverpool Women’s Hospital Campaign. In this post, we are asking our supporters to also support the urgent initiatives from other organisations. The damage to Liverpool Women’s Hospital is symptomatic of all the problems of our NHS, and we fight for the whole NHS.
“As we go marching, marching we battle too for men for they are women’s children and we mother them again”.
The staff and patients are feeling the harm done.
Our local hospitals are in the crisis which we warned about repeatedly, which was predicted, and anticipated. And all the while there were multiple meetings about how to make financial cuts (CIPs),and implement unprecedented (and we think, harmful) financial restrictions and huge reorganisation plans, not to deal with the winter crisis, nor the infant mortality issues, or the gynaecology waiting times, nor birth trauma, but to close services.
The winter crisis was and is avoidable. Capacity should have been built into the system. If Covid taught us one thing it was that we must have emergency capacity. Building capacity means planning well in advance in areas like staffing, in space and equipment, in funding, involving both hospital and community health provision, in action to employ more GPs,in making schools healthier, in mobilising all public services, and if necessary taking over private hospital capacity. Health campaigners have raised this in written and oral questions repeatedly since 2023, more than a year ago. The response was that this winter would be (according to the CEO of the ICB) “…slightly more austere than the previous two years.” The managers of the NHS, nationally and locally, knew what was coming this winter.
The future of Liverpool Women’s Hospital is in grave danger. Please sign our petition here if you have not already done so. Thankfully, LWH is still there and not (yet) fully merged with the other hospitals. Imagine pregnant women in 50 hour waits in A and E, as is happening today in Cheshire and Merseyside.
We raised all this repeatedly with the ICB, but the government made them follow Price Waterhouse Cooper’s cuts agenda, and didn’t that work well ? Fifty damn hours in the A and E!
Do not blame the flu! Do not blame the elders for staying too long in hospital. Privatising social care was a huge blunder. Impoverishing local authorities was a huge blunder.
lobbying the ICB, last winter!!
Save Liverpool Women’s Hospital is one of many organisations fighting to win the NHS back to its true potential, back to being the best in the world.
It is our NHS . Our great grandmothers, and grandfathers fought long and hard for it and won it. For seven decades, we paid for it, invested in it, grew it. For years people voted Labour because of the NHS.
Women hold up half the sky, but 76% of the NHS. The NHS patient facing workforce is massively female, and we thank them for their skill, dedication, humour, and sheer hard graft. The NHS must become a better place to work. Enough is Enough with workplace stress in the NHS. We need more staff and we need to retain those we have. We need education for our NHS to be free.
Women’s health is damaged by more than a decade of neglect.
A Parliamentary report last month spoke of “Medical Misogyny”. The report said women were being left in pain and discomfort that “interferes with every aspect of their daily lives, including their education, careers, relationships and fertility, while their conditions worsen.“
We have a new(ish) Labour Government, after years of deliberate damage to the NHS from the Conservative and Coalition Governments. The trade unions, women’s organisations and the Labour Party fought for universal healthcare, publicly funded, and universally available, and won that battle. The NHS was a major reason to vote Labour as this region did in huge numbers. Yet Labour is throwing vastly more NHS money to the private sector.
We need another mass movement for the NHS to make this government listen.
Privatisation causes pain and harm in healthcare as it has in the railways, in water, in the post office, in royal mail, in telecoms, on the buses, in the power industry, in power, wherever it has touched public services. Private health care in the USA is a cruel, heartless scandal, but it costs the US government twice as much per head as the NHS costs the UK.
We need the billions Streeting is giving to the private sector in our hospitals.
Please sign this petition from “We Own it”. No to billions to the private sector while the NHS struggles.
Private hospitals use the same staff pool as does the NHS. We need more doctors midwives, nurses and other ( fully qualified!) medical professionals in the NHS, not in private hospitals. Private hospitals are not better, not safer, not well regulated, not actually the employers of their surgeons who need private insurance which can randomly be denied.
We oppose privatisation through the new ‘Big Data’ industries. See this shocking post from Keep our NHS Public research about Data.
We say no to privatisation in the NHS, no to the government giving billions to private hospitals. Buy the damn hospitals and put them into proper public service.
What is happening with Liverpool Women’s Hospital in December 2024?
Liverpool Women’s Hospital is under a very serious and utterly ridiculous threat. Please see our suggestions here for how to support keeping the hospital open and better funded on Crown Street. This winter the Royal and Aintree are both overcrowded.
“Stables wanted for the birth of Liverpool babies when they close Liverpool Women’s Hospital”.
Imagine 7,000 babies and their mums and midwives crammed into the already overcrowded Royal? Will our babies be born on the corridors along with the very poorly people?
The fight goes on to Save Liverpool Women’s Hospital as a tertiary hospital on its own site run for women and babies. 76,000 people say so.
We are organising a public meeting with Kim Johnson MP in January and will continue with all the rest of our campaign work. Please help if you can. We especially want to talk to women’s organisations and union branches with big female membership
The future of Liverpool Women’s Hospital is in the balance. There is huge public support for keeping the hospital open and on the Crown Street site, our petition both on line and on paper is growing steadily and is already more than 76,000 signatures.
A Parliamentary report this week spoke of “Medical Misogyny”. The report said women were being left in pain and discomfort that “interferes with every aspect of their daily lives”, including their education, careers, relationships and fertility, while their conditions worsen.“
It also found there to be a “clear lack of awareness and understanding of women’s reproductive health conditions among primary healthcare practitioners” and concluded that gynaecological care is not being treated as a priority.
Pervasive stigma associated with gynaecological and urogynaecological health, a lack of education and “medical misogyny” has contributed to poor awareness of these conditions.
In this situation the closure of the hospital that provides all of Liverpool’s gynaecology care is crazy.
The maternity crisis nationally continues, yet they talk of closing our maternity hospital.
We also keep asking “Where will our babies be born?”
How can we keep a tertiary specialist hospital for women if they close the building, or scatter the services?
There are two big threats.
The trust has formed a committee with Liverpool University Foundation Trust( The Royal Aintree and Broadgreen. We fear that the needs of women and babies will disappear as women’s health and maternity have been neglected in the other big hospitals. So far all the services remain at Crown Street. The first joint meeting has been held. We are not aware of a maternity expert being on this committee. Certainly, men dominate the leading positions.
The ICB is a separate move that has finished an initial “public engagement “ over their plans to for the future of Liverpool Women’s Hospital. This is the first legal step towards closure or merger. We are preparing a detailed response to their plans. At all the public meetings the plans were robustly condemned.
At the ICB board in November we asked
Lobbying the ICB
“Re LWH & Women’s services, re the reporting process from the ‘engagements’ about the future of maternity and Gynaecology services in Liverpool Hospitals.
Why was the ‘independent firm’ not at any of the events? If they are writing the report including those meetings they will only have the ICB reporting on themselves.
How much is the firm getting paid & how much has it cost ICB staff time etc. for these events?
What is the timetable for receiving the results of the report & next steps
How will our petition be recognised by the engagement?
They answered.
As per best practice with an engagement exercise of this sort, NHS Cheshire and Merseyside commissioned an independent organisation – Hood & Woolf – to design and host the engagement questionnaire, collate and analyse responses to it, and to undertake an analysis and report on the feedback across all the different strands of our engagement activity. The report will include a description of the engagement activity undertaken, a summary of the findings, and the key themes, ideas, issues and concerns that have been heard over the six-week period. Analysing data – especially when there are large quantities of qualitative feedback – is a specialist skill, and it is standard practice for us to bring inexternal specialist support to carry this out. Hood & Woolf’s role did not include collecting feedback at engagement events. This is a task routinely carried out by our inhouse team when we are undertaking public engagement, even when the analysis is being supported externally. There was a dedicated note-taker (a member of NHS Cheshire and Merseyside staff) for each of the tables at all events (for the two online events, which had fewer participants, there was a single note-taker who took all the feedback). Their role was to literally take notes of the conversation, not to interpret it in any way. Each original, full set of notes will be provided to Hood & Woolf for them to analyse key themes and areas of discussion, so that this can be summarised in the report. It is important to be clear that the events were only one way in which we were collecting feedback during the engagement. Participants at the events were reminded that even though they had attended an event, it was still important that they completed the main engagement questionnaire. A QR code taking people straight to the questionnaire, and printed versions for those who were not able to complete the questionnaire online, were made available at the events to support this.
Our response to this will be detailed in a later post but we do not think the note-taking was independent or sufficiently detailed.
How much is the firm getting paid & how much has it cost ICB staff time etc. for these events?The core costs for Hood & Woolf’s work are in the region of £24,000.We have not broken down the cost of ICB staff time for this engagement exercise – the work was led by our in-house communications and engagement team, and no additional staffing costs were incurred. However, this has been a significant piece of work for the team, and for others in the organisation, both in terms of planning and delivery. ICBs have a legal duty to involve people, and we are committed to allocating the level of time and resource that this requires. In addition, the Women’s Hospital Services in Liverpool programme is a key organisational priority, and it is critical that we carry out comprehensive engagement with our communities to inform the next stage of work.
What is the timetable for receiving the results of the report & next steps?Work to begin analysing the feedback we’ve received is already underway and will continue over the coming weeks, however it’s important to note that we are still in the process of compiling feedback (for example, questionnaires provided in languages other than English will need to be translated before they can be included). Publishing the report and sharing findings with those who took part in the engagement is an important part of the process, and we plan to do this once the report is finalised and taken through our governance meetings and process. We are likely to be ready to publish the report and details of next steps during March 2025, but we will provide further confirmation on this nearer the time. ( our emphasis)
How will our petition be recognised by the engagement? ( At the last public meeting, the petition was spoken about with disrespect.) The petition was raised and discussed on a number of occasions during the engagement events. We are aware of and have heard the strength of feeling and different views people have shared, and we are grateful for the contributions people have given to our discussions. As stated, the information recorded during table discussions will beanalysed as part of the process of developing the engagement report. With regard to the petition itself, that too will be noted in the engagement report.
The Cheshire and Merseyside Integrated Care Board and the Winter Crisis
In this post, we will report on the winter crisis, and in another post, we will report on their plans for Liverpool Women’s Hospital (both an utter disgrace).
Humans have the “inalienable right to life liberty and the pursuit of happiness”. The right to life must include the right to medical treatment when we are ill.
The NHS must again become a great place to work. NHS staff are working hard in unreasonably difficult situations, overcrowded hospitals are just adding to the crisis. CIPs (cuts)that are being so rigorously imposed must impact on staffing, as 80% of the cost of the NHS is staffing
The Royal College of Nurses say “According to the NMC’s leavers survey, nursing staff cite poor physical and mental health, burnout or exhaustion, and changes in personal circumstances as key reasons for leaving nursing outside of retirement
The BMA say that staff must be supported in this crisis. They have produced a checklist that will help see staff through the winter, if it is all introduced.
1.Communicate honestly with patients about pressures
2 Retain staff and maximise workforce capacity
3.Cut red tape, stop unhelpful targets and barriers and reduce unnecessary bureaucratic workload
4 Taking additional measures to maximising workforce capacity
(This was not mentioned in the ICB response to our questions.)
The ICB is the ruling body of the NHS in Cheshire and Merseyside.
There was no research background to the introduction of these bodies, they are instruments of the privatisation agenda. For more information see here. It is our view that these institutions are not failing but succeeding in aims which are not conducive to good healthcare, aims like cutting services, denying care and remodelling on US corporation lines.
The NHS too often consults private corporations rather than the staff and the public, yet this institution belongs to the people. No one has ever won an election on a promise to privatise or starve the NHS of funds.
The state of our Accident and Emergency departments and the emergency care system in our health service is disgraceful, but the situation has been known about and discussed for many, many months. The years of austerity were supposed to change with the election and the trashing of the Conservative vote, but instead the situation this winter, (according to the CEO of the ICB) “will be slightly more austere than the previous two years”.
NHS Campaigners regularly sit in the public gallery of the ICB, read the papers before the meeting, and ask questions. We have been asking about preparing for and improving the response to the winter crisis for more than a year. We have asked written and oral questions at the ICB meetings. Again and again, the response means we will see once again awful patient, family and staff experiences this winter.
We sent in further questions to the November Board Meeting of the Cheshire and Merseyside ICB about;
The winter crisis,
The Future of Liverpool Women’s Hospital,
Marie Curie Hospice,
At the start of the meeting, the questions are read out and answered. We get a chance to say a little.
Winter comes every single year without fail, so hospitals should not need special arrangements to cope. The preventable deaths, overcrowded hospitals, bursting A and E departments, and the long Ambulance waiting times were entirely predictable and undoubtedly preventable.
Long waits for elective (non-emergency care) are huge 7.5 million cases,(6,341,717 people).Flare ups for these patients send them too into the Accident and Emergency hospitals. Elective care has been funded separately from Acute and Emergency Care but the two kinds of care should never be put into competition with each other. Hopefully, Streeting’s instructions to hospitals to keep patients safe might signal a weakening of the strict demarcation of funding.
In 2023 The Royal College of Emergency Medicine reported that “RCEM estimates that there were almost 14,000 associated excess deaths related to waits of 12 hours or longer in 2023 – more than 268 a week.”
Mr Starmer, the Prime Minister, the person with the power to bring change, quoted those figures in a speech on 12th September 2024. He said “That’s not just a source of fear and anxiety, it’s leading to thousands of avoidable deaths. That phrase ‘avoidable deaths’ should always be chilling. That’s people’s loved ones who could’ve been saved”.
And yet we still face a worse prospect this winter, and it’s not just to do with the flu. By all means, get your flu jab but this situation was predicted at ICB meetings all year.
When we, as members of the public, go to the ICB meetings, we do not expect miracles. We go there to keep the original aims of the NHS alive if only as the voice of protest at what is happening to the NHS, happening this winter of 2024/2025, in our area and others.
The key issues at this meeting were the Liverpool Women’s Hospital, the Winter Crisis, Finance, (which is central to the situation and is hugely troubled), infection control, Celiac products on prescription (yes more cuts), and the shared committee with Lancs and South Cumbria ICB (about closing one of the A and Es in Southport or Ormskirk and meriting 82 mentions in the board papers), and discharge of patients.
For obscure reasons, the merger of 5 Liverpool Hospitals was not discussed.
What we want
We want a publicly owned, Government funded publicly delivered health service for all. Investment in healthcare makes the people, and hence the whole country, healthier wealthier, and happier. We want to return to the Bevan Model of healthcare. The Bevan model is cheaper and more equitable, more cost-efficient but it does not make big profit for the hated US health corporations.
The Bevan model comprises; A universal service, for every human in the country, government-funded, free at the point of need, publicly delivered,providing the best possible treatments.
“It was the first health system in any Western society to offer free medical care to the entire population. It was based on the national provision of services available to everyone.
Aneurin Bevan said “not only is it available to the whole population freely, but it is intended . . . to generalise the best health advice and treatment.”2 The intention was to make the same, high level of service available to all, according to need.”
So why is the NHS in our area, and in others, quite so bad this year?
The NHS today has been harmed by privatisation, the accountable care/ ICB model, and years of deliberate underfunding. When the ICB could not meet its financial targets, Price Waterhouse Cooper was brought in to give advice/ orders on how to reduce spending (make cuts). Price Waterhouse Cooper is a multi-national with significant interest in private health care and a player in the last decade of NHS history. PWC has regular and frequent meetings with the ICB and from the the references in the paperwork, appear to have a major influence.
The influence of PWC goes way beyond Cheshire and Merseyside ICB, they have national influence yet are a private, democratically unaccountable company.
At the start of the ICB meeting, the questions are read out and answered. Written answers are published later on their website. We get a chance to say a little, but enough for them to know the depth of our indignation about the cavalier way lives and dignity can be put at risk.
Our very lives, and the lives of our loved ones, depend on our healthcare, if not immediately then at some time in the future. We value immensely the work done by midwives, nurses, doctors, and all the other NHS workers.
However, in Winter 2024/2025 the damage done to our healthcare by years of austerity is costing lives and damaging our health. People must know what is happening, and how it can be improved.
When people organise together, we can make a difference, we can get change for the better and we can resist harmful change. This is a long-held tradition in Liverpool (but far wider too,) amongst working-class women’s organisations, trade unions and amongst socialists. It is this tradition that led to the founding of the NHS. But campaigners going to these ICB meetings only matter if a wider audience hears about what happens there. So please spread the news we share.
The NHS must be capable of coping with the winter surge in demand but the surge is not in itself caused by the NHS. Our homes are poorly insulated, our heating costs are sky high, many people have not had good healthcare for a long time and people are hard up, good food is expensive and food corporations are allowed to pump out food that overrides normal satiation levels, so its no surprise we get sick in the winter. It’s perfectly predictable and preventable. It is never a surprise. The ICB and the government should be making sure the hospitals can cope.
We have raised this with the ICB since before last winter. Our MPs must be telling the government to release funds to keep our people safe when they are ill.
Years of cuts in the number of beds, hospital closures, of poor workforce planning, have caused real damage. That is the problem, not the season.
These are our questions and their answers from the ICB
Re winter crisis in accident and emergency services
• What has been done to improve the situation from last year?
• Which hospitals face the greatest challenges this year?
The ICB response boils down to
Get patients out of the hospitals as fast as possible.
Stop people coming into the hospitals if there is anywhere else they can go.
Things will be bad.
Put managers into the worst situations (We would prefer that they put in more doctors, nurses, and healthcare assistants before the worst situations arise).
These are some parts of the reply. The full written reply can be seen here.
“It would be misleading to say that winter will pass without some real examples of where the service will fall short in terms of both public and service expectation.”
This is a cosy way of saying some patients and staff will come to harm, and some will die. The responsibility lies squarely with the government. The individuals from the ICB, responding to these questions, might or might not support the policies that lead to these preventable deaths.
“Like many other parts of the country. we have an urgent care system that is facing very real challenges on a daily basis and often falls short in terms of patient and staff experience, and winter only proves to exacerbate those challenges. In previous years additional monies have been provided nationally to provide further resilience but this year there is no expectation of that support. (Our emphasis)……….
“..there are robust improvement programmes which are wrapped around our main acute hospital footprints including primary care, community and mental health providers, and local authorities to tackle issues which manifest themselves within hospitals, most visibly at the emergency department and the ability for ambulance to respond in a timely manner. But we cannot ignore that each of these partner organisations also bear huge operational and clinical pressures……..”
“..during the year there has been significant investment in a new A&E at Arrowe Park, with further investment underway at Macclesfield and the Countess of Chester.”
“It would be misleading to say that winter will pass without some real examples of where the service will fall short in terms of both public and service expectation (our emphasis), and it is difficult to point to one or two hospitals that face the greatest pressure – the reality is that all parts of the system whether it be an acute hospital or other provider face extreme pressure at some time but we do have confidence that after many winters our staff and partners can and will provide the best response possible during this period of intensity”.
The Board is using a new term for corridor care, they call it “Temporary Escalation Spaces.” This is an attempt to normalise a terrible situation.
People who could have been saved will die, and others will suffer pain, discomfort, loss of dignity, and profound anxiety, because the “system” is not adequate for winter, which, after all, comes once a year.
“Theresa May’s plans to introduce means testing for the winter fuel allowance will lead to 3,850 extra pensioner deaths this winter, according to new Labour Party analysis.”
So, after 5 years of further austerity, COVID-19, and huge waiting lists for treatment, most pensioners have now lost their winter fuel payment. We know it is not the same Labour Party as in 2017, but how can they consciously allow possibly even more than 3,500 people to die?
Governments can provide the funds for NHS improvements. Between 2009 and 2020 Governments spent five times the cost of the NHS on ‘Quantitative Easing’ which made the already rich, much richer. Investment in the NHS would help everyone and make the economy grow.
Huge return on Government spending on Healthcare.
Healthcare spending ,when it gets to staff patients and the premises, (not to PWC and the like) gives huge return on the investment, but spending on healthcare in real terms has fallen, including spending per person in the North West.
Our NHS was founded after many decades of campaigning by ordinary working-class women and men, by trade unions, and by socialists. A driving force of the campaigns was to protect our people from unnecessary deaths, and unnecessary pain. The NHS was built to provide healthcare for all, provided by a national, publicly owned, and publicly provided organisation, funded by the government. The successes of the early years of the NHS were stunning. In maternity care there was huge progress, babies survived, and so many more women survived, giving birth.
For more detail on infant mortality please see this.
It is no surprise, therefore, that the NHS is a cherished institution, but it has been very badly damaged for more than a decade by policies and politicians who admire the US system. The ICB system was set up to imitate the Accountable Care Organisations in the USA.
The ICB system was designed to cut services and deny some treatments,
This report describes the NHS contractual system for denial of care, via financial incentives to NHS staff to cut services, which is modelled on the highly profitable operations of UnitedHealth and other US health systems.
The response to the murder of Brian Thompson in New York shows the deep hatred of America’s health system in the states, yet the USA business model is emulated in the NHS (as yet without the public idea of people being charged, quietly though more and more people are paying for their own treatment). We need the people who support universal healthcare, not-for-profit, nationally funded and provided, to get organised.
The NHS is managed at a national level by people deeply intertwined with the US Health system, typified by Simon Stevens, now in the House of Lords, making laws! The NHS management and their financial and political backers are experts at propaganda and sweet talk to hide and make terrible situations sound better.
We say restore and repair the NHS. There is huge support for this across the country. In 2019, when Trump said he wanted the NHS to be part of trade deals, more than 1 million people signed a petition against it.
The “integrated” Care Board is not integrated with social care as it purports to be. Social care is largely privatised, and often charges eyewatering fees to patients and their families. There are some Local Authority reps on the ICB, but the Local Authorities these days are little more than commissioning bodies for social care. Most social care is delivered by privately owned companies, for profit. Initiated by Thatcher, but pushed relentlessly by subsequent Governments, this policy is a disaster for our most vulnerable people.
“In adult social care, 96% of residential services are now outsourced, primarily to for-profit providers”..”Similarly, more than 80% of children’s homes are now run by for-profit companies,“
There are quality issues around these private providers and Co-author, Dr Benjamin Goodair (Department of Social Policy and Intervention, Oxford University) said: ‘Early data suggests that outsourcing has failed to deliver the expected benefits of private sector efficiencies. Instead, the use of profit-driven providers risks worsening care services. As both adult and children’s care sectors face ongoing crises, there is an urgent need for increased scrutiny over the outsourcing of social care.’
For years, the policy has been to close A and E services and cluster them in big hospitals. Southport or Ormskirk look next for the chop as a joint committee of two ICBs has been delegated the decision about their future.
Under funding, cramped conditions and Hospital Acquired Infections
Picture credit to Liverpool Echo last year
Our Acute and Emergency Hospitals are underfunded, understaffed and lack space and beds to treat patients safely. Staff, patients and family members know this from their own experience, but it is backed up by the rise in hospital-acquired infections (as reported on page 95 of the minutes of the Cheshire and Merseyside Integrated Care Board (November 2024).
NICE says ”The National Audit Office has suggested that hospitals with average bed occupancy levels above 85% can expect to have regular bed shortages, periodic bed crises and increased numbers of health care-acquired infections.57 Occupancy rates for acute beds have increased from 87.7% in 2010/11 to 89.5% in 2014/15 so few hospitals are achieving the 85% figure.57 High levels of bed occupancy may affect patient care as directing patients to the bed most suitable for their care is less likely to be possible.
Compared to other nations, the UK has a very low total number of hospital beds relative to its population. The average number of beds per 1,000 people in OECD EU nations is 5, but the UK has just 2.4. Germany, by contrast, has 7.8.
Our hospitals do not have enough beds or enough staff. Consequently patients are discharged as soon as possible but up to 26% can be readmitted within a month
campaigners watching an ICB meeting
The 2023/2024 NHS operational planning guidance recommends that hospital bed occupancy should not exceed 92%. Standards have slipped.
Finances
ICB funding from NHSE England comprises
Core services,
specialised services,
primary care.,
and pharmaceutical, ophthalmic and dental services.
The government and NHSE give the ICB various sums of money. It gives money for elective care, money for such specialist hospitals as have been devolved and money for the routine running of the providers (hospitals and out-of-hospital services, GPs, Dentistry.
Cheshire and Merseyside have the highest funding per head of population of any ICB. Nevertheless, they are in serious financial difficulties, as cuts are imposed Areas for savings/cuts include all age continuing care/complex care, mental health A and E/out of area placements.
The ICB provides the funding for the providers, i.e. the hospitals and organisations providing non-emergency medical care outside of hospitals (like Mersey Care Foundation Trust). The acute and emergency hospitals, and Liverpool Women’s Hospital too, are in financial difficulties. Foundation Trusts technically can go bankrupt which puts them under huge pressure to balance their books at any cost.
“In October, the average handover time for ambulances across England was 40 minutes and 21 seconds” The winter crisis is just one aspect of the damage to the NHS. Maternity, Gynaecology, Mental Health, the GP service, Dentistry all have problems and many are part-privatised.
Services, like audiology, are struggling to cope with the private sector taking the simple cases, leaving the NHS to deal with complex cases and training the next generation of doctors.
Bringing in PAs, and less qualified staff to do some doctors’ roles, is very unpopular and dangerous to life and limb.
It does not have to be this way. A better health service is possible and we need it. Our campaign demands the restoration and repair of our NHS, providing again the best health service in the world and making the NHS the best place to work in the world
We fight for Liverpool Women’s Hospital and to Restore and Repair the NHS.
Day by day, the NHS provides services for patients often with great skill and good humour. Despite years of cuts, the NHS survives but it cannot provide all services we need because of austerity and the privatisation agenda.
We are in grim times, but the fightback is growing. Our petition has reached 76,000 signatures. We have had support to pay for our leaflets and meetings. People who spoke at the engagement meetings unanimously supported keeping Liverpool Women’s Hospital. Not a single member of the public spoke in favour of closing it, or dispersing its services. We have great support from the public, and two Liverpool MPs, Kim Johnson and Ian Byrne, have helped this week. The same day as the ICB meeting and the first joint board meeting of LUHFT and Liverpool Women’s Hospital, Kim Johnson raised the issue in Parliament. Ian Byrne sent a great letter to the Engagement Team, saying “NO!”.
However, the process decided by NHS bureaucrats rolls on. We can stop it if we organise.
The many people who have said “that will never happen” should join the fight back.
Two quotes show the seriousness of the threat we face
At the October 9th meeting of the ICB Fiona Lemens, leading the process said, introducing the engagement, “It’s too early in the process to speculate about how services might look, in the future at the Crown St. site and across the city, because we’ve not started that design work yet, but what we can say is that we need that hospital at Crown St. The things that we could consider that we currently need space for would be out patients, day case procedures. We’ve invested in a CDC, we need that diagnostic capacity for the patients in Liverpool, and this is an excellent building to provide that from and we are absolutely committed to NHS delivered services being delivered from that site, and there are no plans to discuss any other forms of services going in there.”
So, Fiona, where will our babies be born? Where will the women of Liverpool receive their gynaecology care? Where will fertility go? Where will genetics go?Where will the Bradford clinic go?
The website for Liverpool Women’s Hospital says about the second strand in this threat to the integrity of the Women’s Hospital, the largest maternity facility in the country :
“From 1 November 2024, Liverpool Women’s NHS Foundation Trust became part of NHS University Hospitals of Liverpool Group (UHLG). UHLG has been created through the coming together of Liverpool University Hospitals NHS Foundation Trust (LUHFT) and Liverpool Women’s NHS Foundation Trust (LWH).
Please note, Liverpool Women’s Hospital is now represented on the Group Board of Directors of NHS University Hospitals of Liverpool Group (UHLG). Details of past Liverpool Women’s NHS Foundation Trust public board meetings can still be accessed via the links below.“
On Thursday 28th November 2024, two crucial meetings happened. These meetings were:
1) The ICB meeting which received the first report of the Engagement process to decide the future of the Liverpool Women’s Hospital, discussed the winter crisis, and how to handle their lack of adequate funds. We, as members of the public, asked questions. We were told that the first response to the engagement would be reported in February or March. They are paying £24,000 to a company called Hood and Woolf to produce the report on the engagement.
We also learned of the grim financial position, and the situation regarding the terrible winter crisis, likely to be worse than last year. There will be a full report on this in a later post.
2) The inaugural meeting of a new joint committee, which has the delegated powers of the boards of Liverpool Women’s Hospital and the Liverpool University Hospital Foundation Trust (which covers the Royal, Aintree and Broadgreen). We fear that maternity will be treated as badly as maternity has been treated in so many other big acute hospitals, leading to major problems and major enquiries.
This joint committee of LUHT and LWH, also reported that the winter crisis is starting (staff tell us it started a while ago). They also discussed services that might be moved to, or from, the Crown Street site although such moves were already a fait acomplis, and the integrity of a Women’s Hospital seemed to be already lost.
We think it’s wrong that while the ICB follows a protocol to consult on service changes, the merging of the hospitals had no consultation whatsoever, and precious little discussion at the Liverpool Women’s Hospital Board. We were told at the engagement meetings, that merging hospitals does not need public consultation. This huge change was just ‘steamrollered’ through. Merging the Women’s is just the start. The intention is that the specialist hospitals in Liverpool, the Clatterbridge Centre, the Walton Centre and Broadgreen Heart and Chest, will be pulled into an even bigger merger. In contrast to LUHFT, the specialist hospitals have been funded nationally and do not share the financial crises facing LUHFT. It seems odd to us that such major reconfigurations are not considered to require public consultation, while (albeit cruel) changes to such things as celiac prescriptions do. At the ICB it was announced that they are going out to public consultation on whether prescriptions should still be available for gluten-free products for celiacs (A Gluten-free loaf can cost as much as £3.99.) We think this cut is terribly wrong for people already hard up, and struggling for enough food. Many celiacs don’t ask for prescriptions but the damage of this policy will hit the poorest hardest. The Celiac prescriptions cut is yet another cut amongst many – but surely, if this merits consultation, so must merging hospitals?).
Our campaign wants a well-staffed, well-funded Women’s Hospital on the Crown Street site. We want maternity to be funded and staffed well across the UK. We say enough of maternity scandals, enough of birth trauma, and enough of closures and cuts. We say this for all our mothers, daughters, sisters, friends, lovers, and babies. So many other countries do so much better than the UK in maternity and infant mortality. Once we were up with the best but austerity has damaged the service costing many of our babies’ and mothers’ lives, and women’s health.
We have 76,000 signatures on our petition to save Liverpool Women’s Hospital. People sent in many postcards opposing the idea of closure, or dispersal of services as set out in the engagement.
You can read more about the “engagement” process here from Greg Dropkin of Keep Our NHS Public.
We want to restore and repair the whole NHS, and to stop the relentless”Winter Crises”.
The NHS was founded to provide:
A national public service providing healthcare for all, free at the point of need, government-funded, publicly run, and publicly delivered, with well-qualified staff. For decades it worked very well, being declared the best health service in the world. Now it is seriously damaged and must be repaired.
The NHS came from decades of campaigning by working-class women, like the Cooperative Women’s Guild, and the Trade Unions, not from the rich and powerful. If we want to keep it we too fight for it.
The NHS has seen reorganisation after reorganisation in favour of the American model, most recently the Integrated Care Model. The ICB for our area is called Merseyside and Cheshire ICB. This body controls the allocation of money to the hospitals and policy over cuts. Cheshire and Merseyside ICB, and other ICBs simply do not have enough money to function properly. They were conceived as part of a hospital closure project, to reduce the costs of the service and make it more acceptable to US health corporations take-overs. There are other hospital closure plans still going on, as well as the threat to Liverpool Women’s Hospital.
The ICB conducted an “engagement” with the public about the future of Liverpool Women’s Hospital. It was not well publicised but did include four in-person meetings for which they asked people to register. In all four meetings, their proposals were roundly rejected, but the attendance was small, very little effort was put into getting real engagement. We will write more about this in another post. None of the meetings were at a time suitable for working mothers to attend.
What you can do to help
Help with the campaign distribute leaflets and help getting the petition signed.
Raise it with your trade union, or other organisation
Tell your MP and councillor Liverpool Women’s Hospital must stay at Crown Street as a full women’s service run by experts in women’s health, in maternity and related services. Tell your MP that hospitals must cooperate not compete or merge.
Tell them that the winter crisis is unacceptable. Tell them that problems including finance, staffing, buildings and equipment must be sorted and the drain into private companies must stop.
Liverpool Women’s Hospital on the corner of Crown Street and Upper Parliament Street
Campaigners from many organisations say Save Liverpool Women’s Hospital, Restore and Repair the NHS. There are huge problems in the NHS. Maternity and women’s health are just two areas of great concern. In this situation, we say fight for better services, kick out the many privatisation projects, and restore our lost services. Poor, underfunded, fragmented healthcare wrecks a country’s economy, costs lives, and damages individuals and the staff of the service.
This is a quick-fire post responding to questions people have asked about the proposals for the future of Liverpool Women’s Hospital.
Is there really a threat to the future of Liverpool Women’s Hospital? Yes the ICB “engagement” is about Liverpool’s Hospitals’ Maternity and Gynaecological services. There are no other Maternity and Gynaecological services except those at Liverpool Women’s Hospital, so it is about the Women’s Hospital. At the ICB board on the 9th of October, when this “Engagement” was launched, moving all the services from the current site was discussed. This is the link to the “Public Engagement” about the future of Liverpool’s Hospital maternity and gynaecology services. After the “engagement” they will move on to “consultation”. This is part of the closure process and rarely stops, but a big campaign can still stop it.
Where will our babies be born? This plan does not say, but it does discuss moving services from the current hospital. We say “No!!! Save Liverpool Women’s Hospital on the Crown Street site and improve the services there.”
Why do we need women’s health care? Because women’s bodies are different from men’s bodies, because some (but not all) women give birth, because in the UK women’s health has been made worse by austerity, poverty, workplace stress, and pollution. There is a gender health gap. We live longer than men but have more years of ill health, and things are getting worse. It is crucial that women’s health is not subject to more cuts, but rather has massive investment. There is a Liverpool City Council report on women’s health deteriorating in Liverpool up to 2040 here. We campaign for women’s health and for health care for men too.
Where is the money coming from to reorganise women’s health care in Liverpool? There is no mention in the report, nor in the ICB paperwork. Without funding, this is a cut. Liverpool Women’s Hospital has, like other hospitals, been forced to make cuts, they are called ‘cost improvement plans’ but cuts they are, and cannot be made safely. How a massive reorganisation makes sense in this situation of underfunded semi-privatised health care, we do not know. This country can afford world-class healthcare. It is a political choice not to fund healthcare and leave it for the wolves of privatisation who take £10 million a week in profits from our NHS.
Is there money for these plans? No. None has been identified. Both the ICB and Liverpool Women’s Hospitals are underfunded to a serious degree. This is a problem across the NHS but acute for maternity services. For detail see here. Page 56 of the September board meeting gives more detail.
These plans are being led by the ICB. What is the ICB? The ICB is the Cheshire and Merseyside Integrated Care Board. It makes the financial and policy decisions for the NHS in the Cheshire and Merseyside area. The Conservative Health and Care Act 2022 set up forty-two such ICB areas covering the country. Originally they were called Accountable Care organisations. Accountable Care Organisations are an American system. They are intended to cut costs and services, particularly by reducing hospital services. Already this ICB has spent considerably in the private sector.
Is the ICB the same as the Trust? No, but the ICB decides how much money a hospital gets each year and can make policy decisions. A Trust runs hospitals. A trust is the legal body that makes decisions about the hospitals, or in some cases the out-of-hospital services, that it runs. Trusts started in 1991. Then Foundation trusts were brought in in 2004. The idea was that hospitals should run like competing operations. It was a system designed for the private sector to make money. It caused chaos. Lord Darzi’s report has been described as a fig leaf for the government. It describes how bad the situation is so few can now deny the problems. This outright competition is no longer expected, but the laws have not been fully changed. The Government tells National Health Service England what to do, and what it can spend, NHSE then tells the ICBs, and the ICBs tell the hospitals.
What will happen to the site if they take away babies and women? They do not say.
Why do these papers not explain the benefits of Liverpool Women’s Hospital being on a single site? We do not know, but it is a very odd procedure not to include the benefits and costs. The papers do not say what will happen to the Women’s Hospital’s role as a maternal medicine centre for the region, or as a tertiary hospital, which takes complex patients babies and women from other hospitals.
We used to have maternity services available in Fazackerley, Mill Road and Oxford Street. Why close Liverpool Women’s when these services were closed to make way for Liverpool Women’s? We don’t know, and the information published in this report does not make that clear. There were and are advantages to having one maternity hospital and Liverpool Women’s has been good not just for Liverpool women and babies, but as a point of reference for good practice for other Maternity services.
Why the focus on some extremely sick women and not on the thousands of babies born in Liverpool? We do not know. Obviously, sick women and babies are both important.
Staff working at the women’s do not seem to know about this. This is in the public domain. It is not a secret. The plans started ten years ago when the then-head of the CCG (a kind of forerunner of the ICB) announced on Panorama that there were too many hospitals in Liverpool. The next day the Echo said the Liverpool Women’s Hospital was to close. The current documents are similar to the documents produced previously. The original document “Future Generations” formed the basis of the (ridiculously expensive) Carnall Farrar report in 2022, and in turn, this document follows Carnall Farrar.
What’s this about a merger with the Royal, Aintree and Broadgreen? The Royal, Aintree, and Broadgreen formed the Liverpool Universities Hospital Foundation Trust (LUFHT)in October 2019. Liverpool Women’s is now working closely with the LUFT, and sharing a board. That has happened without any public consultation and little discussion at the public meetings of the board. It has not been led by the ICB but by the two trusts. The first joint board meeting is to be this month (November 2024). Legally, the two trusts still exist but have delegated their responsibilities. There was no public consultation on this. The hospitals plan to form a similar committee with the specialist hospitals, Clatterbridge, The Walton Centre and the Liverpool Heart and Chest. For now, it looks like the funding for the specialist hospitals will be ring-fenced, but eventually will be part of the ICB funding system“Today’s NHSE board paper says it will “ringfence” specialised commissioning allocations to ICBs which have the most severe financial problems, including “reserves and discretionary growth funding meaning they could not use it to support other services.” HSJ 7th Dec 2023. However, the joint committee of the hospitals in Liverpool will control finance and staffing for all the hospitals. Where will women’s health stand then? What about our babies? There is a real danger of funding meant for maternity and women’s health being pushed to the background as has happened for a decade nationally.
Can the services just go to the Royal? The Royal has had many problems, not least the loss of beds, ongoing building problems with the new building and the demolition of the old building. There is no room for 7,000 plus babies a year, nor thousands of Gynaecological treatments.
Is there going to be a new building? Highly unlikely, and we think not required. The NHS has a huge problem with building maintenance. Money for buildings is referred to as “capital” to distinguish it from day-to-day spending There is a £13.8 billion backlog, more than the whole capital budget for the year. Darzi’s report said there is a shortfall of £37billion in capital requirements. Some hospitals are practically falling down. Capital spending covers not just buildings but the most expensive equipment, such as intensive care beds (where the UK falls way behind Europe), and robotic surgery, which has excellent results in pain management and length of stay in hospital. Liverpool Women’s Hospital is a good building on a good site.
It is hard to get to Liverpool Women’s Hospital on the bus. What happened to the round the hospitals’ bus service? It was supposed to be every half hour. We are trying to find out. This will be updated when we find out.
How does this address the national maternity crisis? It does not address these issues, which are preventable baby deaths, harm to mothers giving birth and postnatally, funding of staffing, birth trauma for mums and babies, and immense stress for staff. Midwives have made their complaints loud and clear, but despite the many formal hearings into the issues, little progress has been made. Please see here for the list of reports on maternity. None of the hospitals mentioned in these tragic reports were standalone maternity hospitals. The UK does not get into the top twenty countries worldwide for the lowest infant mortality. One in seven maternity units have been closed in the last ten years despite fine talk about choice. The pressure in maternity wards is clear to see.
Is it worse to give birth now than a few decades ago? Yes. Maternal mortality has worsened in the UK. It is now more dangerous to give birth in the UK than it was in in1985 “In the United Kingdom of Great Britain And Northern Ireland, the maternal mortality ratio (per 100 000 live births) has worsened by 1.41 deaths per 100 000 live births from 8.43 [7.66 – 9.26] in 1985 to 9.84 [7.89 – 12.2] in 2020.” (see the link above for details).
Does the report on Liverpool’s hospital maternity and gynaecological services have data or comparators? No comparators, no impact assessment, no equalities assessment, no concrete data, no mention of the dreadful state of maternity finance or the state of the ICB finances. All we are given is unsupported assertions and broad generalisations.
Is the Liverpool Women’s Hospital really “isolated”? No, it is closer, by far, to the Royal,(just one mile down the road) than Broadgreen and Aintree are to the Royal Building or the other two hospitals, even though technically they are one hospital. Liverpool Women’s Hospital has worked as a system with other Cheshire and Merseyside hospitals since the Pandemic through CMAST and has mutual arrangements with other hospitals to operate or collaborate in other buildings, as they should. It is “isolated” in that it is a separate Foundation trust, not part of a bigger hospital but being part of a bigger hospital has far from protected maternity across the country.
Evidence of the financial problems in the ICBLobbying the ICB meeting on the 9th of October2024
Save Liverpool Women’s Hospital campaign was set up after the first attempt to close Liverpool Women’s Hospital nine years ago. We have attended all the public board meetings of the Women’s Hospital and board meetings of the ICB and studied their papers. We have attended conferences, run stalls, produced leaflets, run workshops, and produced this blog. We work closely with other NHS campaigns in Cheshire and Merseyside and nationally. Our campaigners include a range of ages, occupations, women and men, trade union members and pensioners.
For all our sisters,mothers, daughters and babies.












































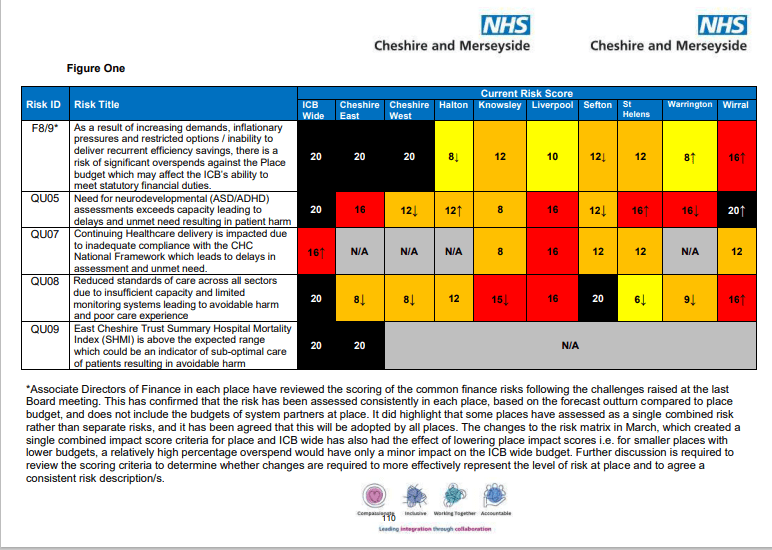



.jpg){kind=link}